Alcohol consumption accounts for 3.2% of the burden of disease and injury in Australia,1 and is second only to tobacco as the greatest preventable cause of drug-related deaths and hospitalisation.2 General practitioners (GPs) play a crucial role in the early detection and management of risky drinking. They have access to the at-risk population, often before the onset of alcohol-related harm.3,4
International and Australian clinical practice guidelines for GPs suggest enquiring about alcohol use regularly, and recommend the routine use of screening questionnaires.5–8 However, GPs have not embraced routine alcohol screening, citing barriers such as the lack of time and resources.9 Importantly, GPs have expressed that alcohol enquiry raises issues relating to the dynamics of the consultation between patient and doctor.10 For instance, they have expressed discomfort with being seen as judgmental or moralising.11–15
Comparatively less is known about patients’ beliefs and attitudes to receiving alcohol enquiry from their GP.16 The context of the consultation (eg reason for presentation) may influence the perceived legitimacy of the alcohol discussions,17–19 but the evidence in this field is slim.20
In this study, we sought to better understand the contexts of these consultations in the Australian general practice setting. First, we tested whether presenting alcohol questions within the SNAP (smoking, nutrition, alcohol, physical activity) framework, recommended by The Royal Australian College of General Practitioners (RACGP),7,8,21 is more acceptable than alcohol-use questions alone. Second, we explored how patients’ acceptability to receiving alcohol enquiry varies according to the common reasons for presentation.
Methods
Study design
We used a survey experiment design22 where participants were randomised to receive one of two postal questionnaires (http://vitualis.com/?page_id=813). The survey responses were then compared and analysed. This study was approved by the University of New South Wales Australia Human Research Ethics Committee (#HC14074).
Participants
Participants were adult patients from a general practice in Sydney, Australia. The clinic is a 35-year-old established teaching practice with five full-time equivalent GPs. The inner-city community has an average age of 35, unemployment at 6.6%, 3.5% identify as Aboriginal and/or Torres Strait Islander, and 25% of households speak two or more languages. Patients were eligible for the mail out if they were older than 18 years of age, and personally attended the clinic for a clinical service during the recruitment week (12 May–18 May 2014). We excluded patients who received clinical services outside of the practice (eg home visits) and those without a valid postal address.
Participants were identified by a search in the clinic’s electronic medical record system (Best Practice Software). This initial list was manually cross-referenced with the practice’s appointment book to ensure accuracy. The census date for questionnaire return was 31 August 2014, 3 months after the initial mail out.
The questionnaires
The intervention (alcohol asked within SNAP) and control (alcohol asked alone) questionnaires began with questions about the patient’s demographic, then assessed alcohol use with the AUDIT-C (Alcohol Use Disorders Identification Test – Consumption).23 The main section of the questionnaires asked participants to rate the acceptability of alcohol enquiry for 20 vignettes of patient presentation to a GP (Table 1). Participants from the intervention group also rated the acceptability of smoking, diet and exercise enquiry. The first 10 vignettes were based on the most frequent patient encounters in Australian general practice.24 The subsequent 10 were based on the most frequent problems managed, excluding repetitions.24
Our vignettes were carefully designed. They were written to a fifth grade (Flesch-Kincaid grade 5.1) student reading level. The language of the vignettes was expressed in the third person to reduce social desirability bias.25 We made use of informal feedback from general practice academic colleagues in the development of the vignettes.
Table 1. List of consultation topics used in the questionnaire vignettes
|
|
Most frequent patient reasons for encounter
|
Most frequent problems managed in general practice
|
|---|
|
1
|
Check-up
|
11
|
Hypertension
|
|
2
|
Prescription
|
12
|
Depression
|
|
3
|
Test results
|
13
|
Diabetes
|
|
4
|
Cough
|
14
|
Arthritis
|
|
5
|
Immunisation
|
15
|
Lipid disorders
|
|
6
|
Throat symptom/complaint
|
16
|
Oesophageal disease
|
|
7
|
Back complaint
|
17
|
Acute bronchitis
|
|
8
|
Administrative procedure
|
18
|
Asthma
|
|
9
|
Blood test
|
19
|
Anxiety
|
|
10
|
Rash
|
20
|
Urinary tract infection
|
Outcomes
The acceptability of GPs’ alcohol enquiry was rated in each vignette using a labelled 6-point Likert scale. These ratings were transformed into three categories (unacceptable, ambivalent and acceptable), each representing two adjacent points on the scale for analysis. The primary outcome measured was the number of vignettes, rated as acceptable, per questionnaire. Individual vignette ratings were tabulated to explore how acceptability varied according to the reason for the encounter.
Sample size
The sample size was determined a priori. The study was designed to detect a small–moderate effect (Cohen’s d = 0.35)26 on the primary outcome, using a two-tailed independent samples t-test (power = 0.8, α = 0.05). The sample size required was 260 and we aimed to recruit 400 participants, assuming a 65% response rate.
Randomisation
An online randomisation service (www.sealedenvelope.com) was used to generate the group allocation sequence. Random block sizes of 4, 6 and 8 were used. The sequence was applied to an alphabetised list of participants to create the groups.
Statistical analyses
The mean number of vignettes rated as acceptable was compared between the groups, and expressed as an estimate with 95% confidence intervals and in Cohen’s d. Significance was tested using t-test.
The acceptability of alcohol enquiry to individual vignettes was ranked and is reported descriptively. Spearman’s correlation coefficient (rs) was used to determine the consistency of these vignette rankings between groups.
The demographics of the participants are reported descriptively and differences between the groups were analysed using t-test and chi-square. Statistical analyses were performed using International Business Machines (IBM) Corporation SPSS Statistics 22 software.
Results
Participants
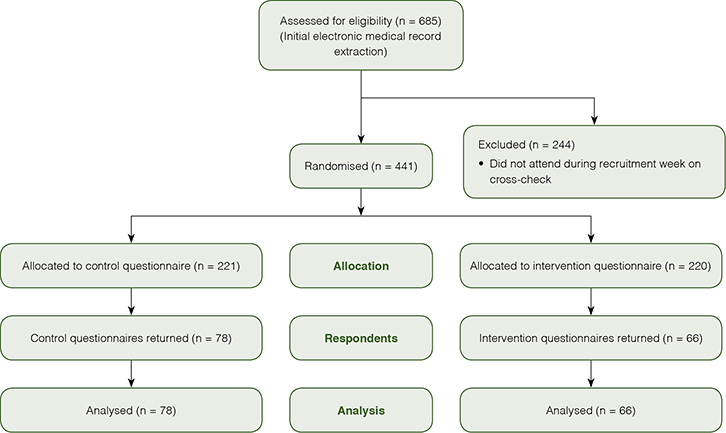 |
| Figure 1. Study participant flow |
An initial search of the electronic medical record database for adults consulted during the recruitment week resulted in identification of 685 patients (Figure 1). After excluding individuals who had not actually visited the clinic (eg correspondence imported, telephone calls), 441 patients (299 women, 142 men) were recruited. Participants were randomised and included in the mail out. The mean age was 50.5 years and the age range was 18.5–95.2 years.
There were 144 questionnaire respondents (32.7%), 78 and 66 from the control and intervention groups respectively. The responding participants tended to be older than those in the mail out (53.8 vs 50.5 years, P = 0.055). In brief, most of the respondents were married (66.0%), Australian-born (70.8%), university educated (64.6%) and an existing patient of the clinic (81.7%); and 36.4% were classified as risky drinkers (Table 2).
The two groups were very similar, though participants in the intervention group were more likely to have been born outside of Australia or the UK (27.3% vs 11.5%, P = 0.048), and were more likely to have been a new patient of the clinic (25.8% vs 11.8%, P = 0.049).
Table 2. Survey respondents’ demographics
|
|
Participant characteristics
|
Total
|
Control group
|
Intervention group
|
Significance*
|
|---|
|
Number
|
n
|
144
|
78
|
66
|
|
|
Sex
|
Male – n (%)
|
47 (32.9)
|
24 (31.2)
|
23 (34.8)
|
P = 0.722†
|
|
Female – n (%)
|
96 (67.1)
|
53 (68.8)
|
43 (65.2)
|
|
Age
|
Mean – year (range)
|
53.8 (20–91)
|
52.9 (20–88)
|
53.6 (20–91)
|
P = 0.899‡
|
|
Standard deviation
|
17.3
|
17.3
|
17.7
|
|
Married or regular
partner
|
Yes – n (%)
|
95 (66.0)
|
54 (69.2)
|
41 (62.1)
|
P = 0.384†
|
|
No – n (%)
|
49 (34.0)
|
24 (30.8)
|
25 (37.9)
|
|
Country of birth
|
Australia – n (%)
|
102 (70.8)
|
61 (78.2)
|
41 (62.1)
|
P = 0.048†
|
|
United Kingdom – n (%)
|
15 (10.4)
|
8 (10.3)
|
7 (10.6)
|
|
Other – n (%)
|
27 (18.8)
|
9 (11.5)
|
18 (27.3)
|
|
Aboriginal person
|
Yes – n (%)
|
3 (2.1)
|
0 (0)
|
3 (4.5)
|
P = 0.094†
|
|
No – n (%)
|
141 (97.9)
|
78 (100)
|
63 (95.5)
|
|
Highest level of education
|
High school – n (%)
|
51 (35.4)
|
30 (38.5)
|
21 (31.8)
|
P = 0.485†
|
|
University – n (%)
|
93 (64.6)
|
48 (61.5)
|
45 (68.2)
|
|
Employment status
|
Employed – n (%)
|
68 (47.2)
|
33 (42.3)
|
35 (53.0)
|
P = 0.516†
|
|
Student – n (%)
|
8 (5.6)
|
6 (7.7)
|
2 (3.0)
|
|
Unemployed – n (%)
|
4 (2.8)
|
2 (2.6)
|
2 (3.0)
|
|
Retired – n (%)
|
33 (22.9)
|
20 (25.6)
|
13 (19.7)
|
|
Pension – n (%)
|
24 (16.7)
|
14 (17.9)
|
10 (15.2)
|
|
Parental leave – n (%)
|
2 (1.4)
|
0 (0)
|
2 (3.0)
|
|
Domestic duties – n (%)
|
5 (3.5)
|
3 (3.8)
|
2 (3.0)
|
|
Is a new patient
|
Yes – n (%)
|
26 (18.3)
|
9 (11.8)
|
17 (25.8)
|
P = 0.049†
|
|
No – n (%)
|
116 (81.7)
|
67 (88.2)
|
49 (74.2)
|
|
GP visits in past year
|
Mean (n)
|
8.3
|
9.1
|
7.6
|
P = 0.379‡
|
|
Standard deviation
|
9.7
|
11.4
|
7.3
|
|
Median
|
6
|
6
|
6
|
|
No of regular
medicines
|
Mean (n)
|
2.7
|
3.1
|
2.3
|
P = 0.079‡
|
|
Standard deviation
|
2.7
|
3.1
|
2.2
|
|
Median
|
2
|
2
|
2
|
|
Drinker status§
|
Non-drinker – n (%)
|
27 (19.3)
|
14 (18.7)
|
13 (20.0)
|
P = 0.951†
|
|
Low-risk – n (%)
|
62 (44.3)
|
34 (45.3)
|
28 (43.1)
|
|
Risky – n (%)
|
51 (36.4)
|
27 (36.0)
|
24 (36.9)
|
|
*Where appropriate, the test is between the control and intervention groups
†Pearson Chi-Square (exact significance), 2-sided
‡Independent samples t-test, equal variance not assumed, 2-tailed
§Risky drinker: AUDIT-C score ≥5 in men, and ≥4 in women24
Note, in some cases, the numbers do not add up to the totals for a given column, as not all respondents answered all questions
|
Primary outcome – GPs’ alcohol enquiry acceptability
The mean number of vignettes where GPs’ alcohol enquiry was rated as acceptable by the control group was 14.1, compared with 16.2 by the intervention group (Table 3).
This is a small-to-moderate, statistically significant effect favouring the intervention.
To determine whether country of birth or new patient status confounded this result, we used two-way factorial analysis of variance (ANOVA) to test for interactions between these demographic factors and participant group allocation, for the primary outcome measure. There were no statistically significant interactions (participant group × country of birth, P = 0.537; Participant group × New patient status, P = 0.404).
Table 3. Primary outcome comparison
|
|
Group
|
n
|
Mean (SD)
|
Mean difference
|
95% confidence interval
|
Effect size*
|
Significance†
|
|---|
|
Control
|
78
|
14.1 (5.8)
|
2.1
|
0.4–3.7
|
d = 0.40
|
P = 0.016
|
|
Intervention
|
66
|
16.2 (4.3)
|
|
Primary outcome measure (dependent variable) is number of vignettes per questionnaire where GP alcohol enquiry is rated as acceptable (range 0–20)
The independent variable is group allocation
*The mean difference expressed in Cohen’s d
†Independent samples t-test, equal variance not assumed, 2-tailed
|
GPs’ alcohol enquiry acceptability by scenario
The acceptability of receiving GPs’ alcohol enquiry in the individual vignettes varied markedly (Table 4). The acceptability rank of the vignettes was consistent between the responses of the control and intervention groups (rs = 0.89, P < 0.001).
Table 4. Order of acceptability of GP alcohol enquiry by scenario vignette
|
|
Acceptability rank order
|
Control questionnaire group (%)
|
Intervention questionnaire group (%)
|
|
|
#
|
Scenario vignette
|
Unacceptable
|
Ambivalent
|
Acceptable
|
Unacceptable
|
Ambivalent
|
Acceptable
|
|
1
|
Diabetes
|
1.3
|
7.7
|
89.7
|
1.5
|
1.5
|
97
|
|
2
|
Oesophageal
disease
|
2.6
|
10.3
|
85.9
|
0
|
1.5
|
98.5
|
|
3
|
Hypertension
|
1.3
|
10.3
|
87.2
|
1.5
|
1.5
|
97
|
|
4
|
Depression
|
2.6
|
7.7
|
88.5
|
0
|
4.5
|
95.5
|
|
5
|
Check-up
|
6.4
|
9
|
84.6
|
0
|
4.5
|
95.5
|
|
6
|
Lipid disorders
|
1.3
|
12.8
|
84.6
|
1.5
|
3
|
95.5
|
|
7
|
Anxiety
|
5.1
|
5.1
|
88.5
|
6.1
|
7.6
|
86.4
|
|
8
|
Blood test
|
2.6
|
21.8
|
73.1
|
6.1
|
12.1
|
81.8
|
|
9
|
Asthma
|
6.4
|
17.9
|
73.1
|
4.5
|
13.6
|
78.8
|
|
10
|
Arthritis
|
2.6
|
28.2
|
67.9
|
4.5
|
12.1
|
83.3
|
|
11
|
Urinary tract
infection
|
2.6
|
26.9
|
69.2
|
3
|
18.2
|
78.8
|
|
12
|
Rash
|
11.5
|
21.8
|
65.4
|
4.5
|
13.6
|
81.8
|
|
13
|
Acute bronchitis
|
6.4
|
25.6
|
66.7
|
6.1
|
16.7
|
77.3
|
|
14
|
Prescription
|
11.5
|
21.8
|
66.7
|
7.6
|
19.7
|
72.7
|
|
15
|
Test results
|
6.4
|
26.9
|
65.4
|
9.1
|
19.7
|
71.2
|
|
16
|
Cough
|
14.1
|
26.9
|
59
|
4.5
|
21.2
|
74.2
|
|
17
|
Throat symptom
|
15.4
|
35.9
|
48.7
|
7.6
|
18.2
|
74.2
|
|
18
|
Immunisation
|
19.2
|
28.2
|
51.3
|
18.2
|
22.7
|
59.1
|
|
19
|
Administrative procedure
|
23.1
|
26.9
|
50
|
25.8
|
16.7
|
57.6
|
|
20
|
Back complaint
|
21.8
|
32.1
|
46.2
|
15.2
|
24.2
|
60.6
|
|
Spearman’s correlation coefficient (2-tailed), rs = 0.89, P <0.001
|
Discussion
These results suggest alcohol-use assessment is perceived to be more acceptable by general practice patients when it is conducted within the SNAP framework. The effect was small-to-moderate in size, but clearly consistent across the presenting scenarios (Table 4).
Although this may not be surprising to Australian GPs, to our knowledge it is the first time it has been demonstrated experimentally. Our findings support the RACGP’s SNAP-based approach to behavioural risk factor management.7,8,21
Our study also substantiates the notion that the reason for presentation has an important influence on GPs’ alcohol enquiry acceptability. For instance, while the majority of participants found alcohol enquiry acceptable in the diabetes vignette, only half found it acceptable in the back complaint (written as acute back pain) vignette. Interestingly, up to one-fifth of participants rated GPs’ alcohol enquiry as ‘unacceptable’ in that vignette. These results are consistent with the qualitative literature available on patients’ beliefs and attitudes to alcohol discussions in general practice. Acceptability has been reported to be contingent to an ‘appropriate context’.17,19
There are a number of important implications for the practice of early detection of risky drinking in primary care. First, it has often been assumed that ‘research demonstrates that patients generally have positive views towards discussing alcohol with PHC [primary healthcare] professionals’.27 However, it is likely the surveys that form this research do not capture important situational contexts and patient reservations that occur in general practice consultations.19,28 The implicit demand for fidelity to universal alcohol-screening procedures29 might be inappropriate, or at least unrealistic, unless implementation can take into account patients’ values and preferences.
Second, alcohol screening might be more acceptable overall if the tools and instruments were integrated within a holistic lifestyle assessment framework, with development that made use of patients’ and GPs’ perspectives.16 For instance, New Zealand researchers have reported high acceptability of the eCHAT (electronic Case-finding and Help Assessment Tool), where patients self-administer a lifestyle and mental health screening tool on an iPad in the waiting room, and indicate whether they would like help with the screened issue.30
Strengths and limitations
Our vignettes covered the most common Australian general practice presentations, were easily understood and sought to reduce bias from socially desirable responses. Importantly, by using the experimental rather than cross-sectional survey approach, we were able to make causal inferences.22 As our participants were randomised and blinded to the alternative questionnaire, it is likely the differences in responses between the groups are real and attributable to independent variable.
Although there are some data that suggest survey experiment results do correspond to actual behaviours,31 this is an area of some debate.32 We acknowledge the external validity of our results to real consultations is unknown.
The survey response rate was also lower than expected, but nonetheless, our primary outcome comparison reached statistical significance, partly as the measured effect size was larger than the assumption in our power calculation. However, it is possible the participants have beliefs and attitudes that do not represent the practice patient population. The participants were found to be older, Australian-born and especially well-educated. As the study was conducted in a single centre, the participants’ demographics were narrow. It is unclear how well our results reflect the views of broader multicultural Australian society.
Lastly, our survey method does not inform us of the reasons underlying participant responses. The subsequent qualitative section of our research project will augment these survey results.
A direction for further research is to capture the beliefs and attitudes of patients from diverse cultural backgrounds. Sociocultural beliefs surrounding alcohol use appear to be a key barrier to GPs detecting risky drinking.10 It is important to explore this from patients’ perspectives.
Implications for general practice
- Patients may find alcohol-use assessment in general practice to be more acceptable when it is framed within the SNAP framework.
- Consultations about diabetes, gastro-oesophageal reflux, hypertension and depression provide good opportunities for GPs to ask about alcohol. Patients appear to perceive enquiry in these contexts as especially acceptable.
Acknowledgements
The authors thank the patients who participated in the study. We especially acknowledge Ms Jacqui Ellsmore and Ms Wendy Liu for support with the questionnaires at the general practice, Ms Sarah Jacob for organisational support of the project and Ms Janice Tan for assistance with the mail out and data entry. Lastly, this project was funded by an RACGP Family Medical Care, Education and Research Grant and the authors gratefully acknowledge the RACGP Foundation for their support.
Authors
Chun Wah Michael Tam BSc(Med) MBBS MMH(GP) FRACGP, Staff Specialist in General Practice, General Practice Unit, Fairfield Hospital, Prairiewood, NSW; Conjoint Senior Lecturer, School of Public Health and Community Medicine, University of New South Wales, Sydney, NSW. m.tam@unsw.edu.au
Louis Hion-Lam Leong, medical student, Medicine, University of New South Wales, Sydney, NSW
Nicholas Zwar MBBS, MPH, PhD, FRACGP, Professor of General Practice , School of Public Health and Community Medicine, University of New South Wales, Sydney, NSW
Charlotte Hespe MBBS (Hons), DCH, GCUT, FRACGP, FAICD, Head, General Practice Research and conjoint Head, General Practice, School of Medicine, University of Notre Dame Australia, NSW
Competing interests: The authors received funding for this project from an RACGP Family Medical Care, Education and Research Grant.
Provenance and peer review: Not commissioned, externally peer reviewed.