Ingrown toenails
The article by Bryant and Knox (AFP March 2015)1 rightly concluded that the choice of technique to treat an ingrown toenail is largely dependent on the practitioner’s experience and preference. Having tried both the techniques described, I am surprised they gave equal prominence to nail fold excision and matrixectomy. In my experience, surgical excision runs a distant second when it comes to post-operative comfort and speed of healing. Excising an infected nail fold, then incising a healthy nail bed and suturing it under tension is contrary to basic surgical principles.
An article on ingrown toenails in American Family Physician2 detailed excision of the lateral nail plate combined with lateral matrixectomy as providing the best chance for eradication. The lateral 3 mm of the toenail is avulsed and the corresponding germinal matrix is obliterated by electrocautery, phenol cautery or excision with a small scalpel. Access to the germinal matrix under the proximal nail fold is through a 1 cm incision in the same line as the nail split, which can be closed with a sterile adhesive strip.
Granulation tissue in the nail fold should be curetted away, but no incision is made through either the nail fold or the nail bed. No pain relief is required and normal activities can resume the next day after this conservative procedure, as opposed to often a week or more after the Winograd surgical procedure. I have found recurrence of an ingrown toenail to be extremely rare after this matrixectomy procedure.
Dr Dennis Chambers
Adelaide, SA
Reply
Dr Chambers describes an alternative approach to the surgical management of an ingrown toenail. The approach offers three methods of matrix ablation – electrocautery, sharp excision and the application of phenol BP – through a 1-cm incision. We agree with Dr Chambers that ‘excising an infected nail fold, then incising a healthy nail bed and suturing it under tension is contrary to basic surgical principles’. This was not advocated in our article.
As the article described, treatment of an infected ingrown toenail should include removal of the offending nail edge and hypergranulation tissue, followed by appropriate soaks and/or antiseptic dressings, with antibiotics being prescribed if clinically indicated.
The technique referred to by Dr Chambers may well be an efficacious procedure in experienced hands, but it is not as well supported with published clinical data as the Winograd or phenol matrixectomy procedures. Our article referenced clinical research that included a minimum follow-up period of 10 months, which is an adequate time frame to allow for nail re-growth.
Authors
Prof Alan Bryant BSc (Pod), MSc, PhD,
Professor and Head, Podiatric Medicine Unit,
School of Surgery, Faculty of Medicine, Dentistry and Health Sciences,
University of Western Australia,
Crawley, WA
Andrew Knox BPodM, Assistant Professor,
Podiatric Medicine Unit, School of Surgery,
Faculty of Medicine, Dentistry and Health Sciences,
University of Western Australia,
Crawley, WA
Scurvy not rare
The report by Wong et al3 of a clinical case of rash due to scurvy is an important reminder to consider the diagnosis of scurvy in contemporary Australian medical practice. We agree with the concern that scurvy may not be a rare condition and may be more prevalent in the community than is widely believed.
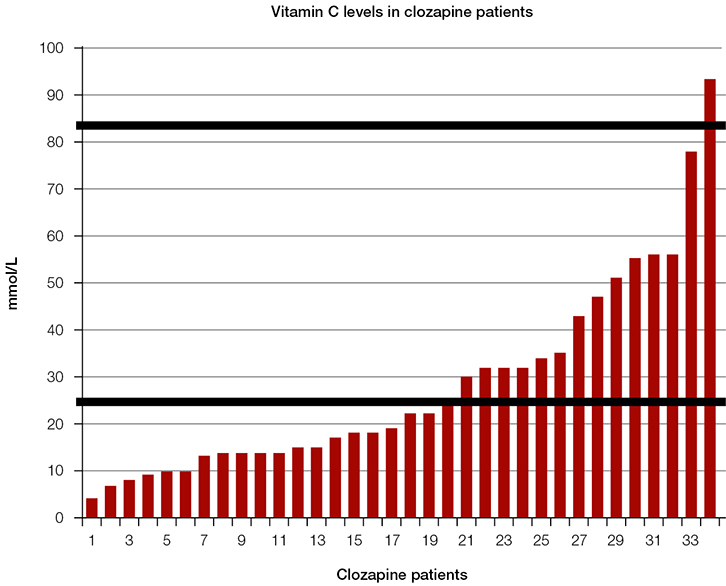 |
| Figure 1. Vitamin C levels in clozapine patients |
Vitamin C depletion was present in the majority (>50%) of a cohort of patients in a clozapine clinic in South Australia in 2013 (Figure 1). Four cases of scurvy recently (December 2013–February 2014) presented to my general medical practice (Table 1).
Table 1. Clinical cases of scurvy in December 2013–February 2014
|
|
Demographics
(age, sex)
|
Clinical features
|
Risk factors
|
Vitamin C
(reference 26–85 μmol/L)
|
|---|
|
73, F
|
- Fatigue
- Weight loss
- Hypotension
|
- Anxiety and depression
- Financial stress
|
9
|
|
31, M
|
- Fatigue
- Nausea and vomiting
- Rash
|
- Schizophrenia
- Financial stress
|
7
|
|
31, M
|
- Fatigue
- Peri-rectal bleeding
- Diarrhoea
- Muscle cramps
- Rash
|
- Homeless
- Financial stress
|
15
|
|
56, F
|
- Fatigue
- Acute coronary syndrome
|
- Depression
- Financial stress
|
4
|
Unfortunately, Australian nutritional surveys have not included measures of vitamin C. Therefore, the prevalence of deficiency in this country is unknown. Community rates of vitamin C deficiency internationally were found to be 8–25% for men and 6–16% for women.4–6 Disadvantaged groups are at particular risk. It was found 95% of individuals in a population of those experiencing homelessness in Paris were vitamin C-deficient.7
Considering a clinical trial that established an effective treatment for scurvy was conducted in 1747,8 the occurrence of scurvy in Australia in 2014 represents an evidence practice gap of more than 250 years. This is unfortunate.
Dr Genevieve Gabb General Medicine,
Royal Adelaide Hospital Adelaide, SA
Dr Bronte Gabb,
Senior Medical Practitioner Psychiatry,
Noarlunga Health Service,
Noarlunga Hospital Noarlunga, SA
References
- Wong C, Lyons G, Nicolopoulos J, Varigos G. A rare cause of petechial rash in the 21st century. Aust Fam Physician 2014;43:853–55.
- Mosdol A, Erens B, Brunner EJ. Estimated prevalence and predictors of vitamin C deficiency within UK’s low-income population. J Public Health (Oxf) 2008;30:456–60.
- Schleicher RL, Carroll MD, Ford ES, Lacher DA. Serum vitamin C and the prevalence of vitamin C deficiency in the United States: 2003-2004 National Health and Nutrition Examination Survey (NHANES). Am J Clin Nutr 2009;90:1252–63.
- Hercberg S, Preziosi P, Galan P, et al. Vitamin status of a healthy French population: Dietary intakes and biochemical markers. Int J Vitam Nutr Res 1994;64:220–32.
- Malmauret L, Leblanc JCh, Cuvelier I, Verger Ph. Dietary intakes and vitamin status of a sample of homeless people in Paris. Eur J Clin Nut 2002;56:313–20.
- Lind J. A treatise of the scurvy. In three parts. Containing an inquiry into the nature, causes and cure, of that disease. Together with a critical and chronological view of what has been published on the subject. Edinburgh: A Millar, 1753.
Letters to the Editor
Letters to the Editor can be submitted via:
Email: afp@racgp.org.au
Mail: The Editor, Australian Family Physician
100 Wellington Parade East Melbourne VIC 3002 Australia