Case
A woman, 62 years of age, presented to a general practice with a three-day history of persistent double vision. She described this as ‘seeing two images side by side’. There was no previous history of diplopia or trauma, headache, vomiting, limb weakness or jaw claudication. She could not remember the last time she saw a medical practitioner. She was not on any regular medications. There was no family history of diabetes, hypertension or ischaemic heart disease.
Clinically, her blood pressure was 152/79 mmHg and pulse was regular at 87 beats per minute. Her weight was 75 kg and height was 155 cm, making her body mass index (BMI) 31 kg/m2. Examination revealed right-eye esotropia and diplopia in the primary gaze (Figure 1). Her diplopia disappeared on closing either eye. It was worse at the right lateral gaze with restricted right eye abduction (Figure 2). Other extraocular movements were normal with no pain. The diplopia was also worse with distance fixation. Her pupils and eyelids were normal to examine. Visual acuity was 6/6 and 6/9 for the right and left eye respectively. Fundoscopic examination was unremarkable. Other cranial nerve and neurological examinations were unremarkable. Capillary blood glucose was 5.6 mmol/L.
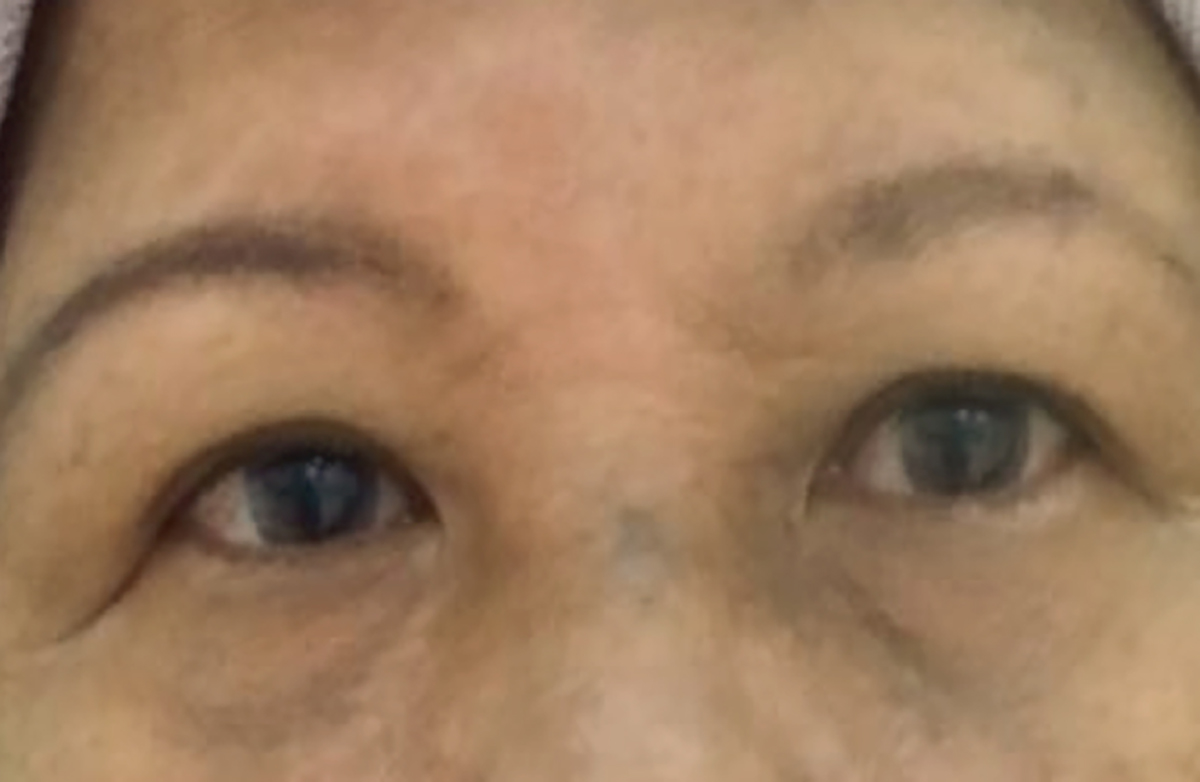
Figure 1. Patient in primary gaze

Figure 2. Patient in right gaze
Question 1
What is the first thing to determine when a patient presents with diplopia?
Question 2
What are the causes of binocular diplopia?
Question 3
What is the diagnosis at this point?
Question 4
What are the potential causes of the diagnosed condition?
Answer 1
The first thing to determine when a patient presents with diplopia is identifying whether it is monocular or binocular. Binocular diplopia disappears when one eye is occluded. Monocular diplopia usually suggests a refractive problem at the front part of the eye, such as astigmatism or cataract.
Answer 2
The causes of binocular diplopia include:
- cranial – isolated cranial nerve III, IV or VI palsy, combined cranial neuropathy (if lesion in cavernous sinus or brainstem)
- neuromuscular – myasthenia gravis, botulism
- muscular – thyroid eye disease, orbital myositis, tumours, trauma, myopathies (eg chronic progressive external ophthalmoplegia, myotonic dystrophy).
Answer 3
The diagnosis at this point of the consultation would be right isolated abducens (cranial nerve VI) palsy.
Answer 4
The causes of abducens (cranial nerve VI) palsy include:1
- microvascular (8–36%)
- neoplastic (39–45% in series of children)
- traumatic (5–20%).
The most common cause in those aged >50 years is microvascular ischaemia, but it is important to consider this palsy as a false localising sign for raised intracranial pressure.
Case Continued
The patient’s case was discussed with an ophthalmologist, who agreed with outpatient investigations, and arranged to see her the next working day with the results.
Question 5
What investigations should be considered?
Answer 5
Investigations to consider include:
- full blood examination (FBE)
- erythrocyte sedimentation rate (ESR)
- thyroid function tests (TFTs)
- fasting glucose and lipids
- magnetic resonance imaging (MRI) of the brain with gadolinium.
Case Continued
Ophthalmology review confirmed the initial ocular examination findings. The optic disc and retinal vessels were normal. All of the blood tests were within normal limits except for total cholesterol and low-density lipoprotein-cholesterol (LDL-C), which were 6.6 mmol/L and of 4.7 mmol/L respectively. The MRI of her brain showed mild, small vessel ischaemic changes at the white matter of bilateral cerebral hemispheres, with no other abnormalities.
Question 6
What is the diagnosis now?
Question 7
What are the next steps in management?
Answer 6
Given the investigation results for this patient, the diagnosis is ischaemic right abducens (cranial nerve VI) palsy.
Answer 7
The patient was advised to patch the affected eye for temporary relief of her diplopia.
Conclusion
On review at six weeks, the patient reported that the diplopia was less severe and there was just slight restriction on right gaze. On subsequent review at 12 weeks, her symptoms improved significantly. Diplopia on primary gaze had resolved. There was only a small-angle diplopia on right gaze despite full extraocular movements. Her cardiovascular risk factors, including hyperlipidaemia and hypertension, were managed concurrently.
Discussion
There are differing opinions with regard to brain imaging in acute isolated ocular motor nerve palsies for patients with characteristics similar to this case (aged >50 years with microvascular risk factors). Some suggest observation without neuroimaging unless there is no spontaneous resolution by three to six months.2–8 The argument is that microvascular infarction is a common cause for this category of patients and it typically resolves spontaneously over 10–12 weeks.1 Murchison et al2 recommend a brain MRI only if the patient is aged <50 years, has a history of malignancy, lack of neurological isolation of the palsy, or has no resolution at three months.
Others advocate for immediate brain MRI to be performed during the initial evaluation of all adults.1,9–15 The authors of this article favour this approach. In about 17% of cases from two different studies,11,13 alternative diagnoses to microvascular palsy that can change the acute management and long-term prognosis of patients were discovered. These include brainstem infarction, demyelinating disease and neoplasm.11,13 A computed tomography (CT) scan can be helpful to rule out large neoplasms where MRI services are unavailable.
Key points
- When assessing diplopia, first determine whether it is monocular or binocular.
- Always perform a fundoscopic examination in a patient with abducens (cranial nerve VI) palsy as this nerve is very susceptible to increased intracranial pressure.
- An MRI of the brain has an important role in evaluating a patient with an abducens (cranial nerve VI) palsy. However, at the time of writing, this is not covered by Medicare for general practitioner (GP) referrals for this indication.
- Ophthalmology or neuro-ophthalmology consultation is recommended for further assessment and management.
Authors
Mohamed-Syarif Mohamed-Yassin, MBBS, FRACGP, DipPallMed (Clin), Family Medicine Specialist, Faculty of Medicine, Sungai Buloh Campus, Universiti Teknologi MARA, Selangor, Malaysia. syarif.yassin@gmail.com
Noorhida Baharudin MBBS, FRACGP, Family Medicine Specialist, Faculty of Medicine, Sungai Buloh Campus, Universiti Teknologi MARA, Selangor, Malaysia
Norasyikin Mustafa MBChB, MOphthal, Ophthalmologist, Faculty of Medicine, Sungai Buloh Campus, Universiti Teknologi MARA, Selangor, Malaysia
Competing interests: None.
Provenance and peer review: Not commissioned, externally peer reviewed.