Nasal obstruction can be defined as a subjective sensation of insufficient airflow through the nasal cavity and can be anatomical, physiological or of combined aetiology. Similarly to respiratory mucosa, the nasal mucosa is affected by local and systemic mediators.
Normal nasal anatomy
The nasal cavity commences at the external nasal valve, which is defined by the lower lateral cartilages, inferior septum, nostril sill and alae. Superiorly, the septum and nasal bones provide the structural support of the nose. The septum is the midline structure that separates the two nostrils and is composed of cartilage anteriorly and bone posteriorly. The internal nasal valve is the narrowest aspect of the nasal cavity and is formed by the septum, inferior turbinate and upper lateral cartilage on either side. There are three turbinates (superior, middle and inferior) that arise from the lateral nasal wall; their function is to humidify, warm and filter air (Figure 1A). Inferolateral to each turbinate is a corresponding meatus into which the paranasal sinuses and nasolacrimal duct open.1
Clinical presentation
Patients with nasal obstruction typically report a sensation of fullness or stuffiness in the nasal airway. When experienced at night, this can adversely affect quality of sleep, resulting in daytime somnolence and fatigue.2,3 Other associated symptoms include:
- Rhinorrhoea – this can be clear or purulent. Clear rhinorrhoea is associated with allergic and non-allergic rhinitis. Unilateral clear rhinorrhoea raises the suspicion of cerebrospinal fluid (CSF) leak. Purulent rhinorrhoea may indicate an infective aetiology.
- Facial pain – this may be experienced in the context of acute sinusitis but is unusual in chronic rhinosinusitis. Acute sinusitis may also be associated with fever. There is a long list of differential diagnoses for facial pain (including bruxism, atypical migraine and radiation for cervicogenic aetiology and neuropathic pain) and in the absence of other symptoms suggestive of acute sinusitis other causes should be considered.
- Alteration in the sense of smell and taste – this may indicate nasal polyps and/or chronic rhinosinusitis.
- Atopic features – pruritus, epiphora and sneezing – are more prominent in allergic than non-allergic rhinitis. A history of asthma or dermatitis is more likely in the context of allergic rhinitis.
Clinical assessment
The differential diagnosis of nasal obstruction is broad and refined by a focused history and examination (Box 1).
Box 1. Causes of nasal obstruction
|
Common
Rhinitis:
- Allergic
- Non-allergic (infectious/vasomotor/rhinitis medicamentosa)
Chronic rhinosinusitis with or without nasal polyposis
Inferior turbinate hypertrophy
Septal deviation
Adenoid hypertrophy
Dry nasal mucosa
Medications:
- Antithyroid medication
- Oral contraceptives and other oestrogens
- Antihypertensive agents (beta blockers, calcium channel blockers, angiotensin converting enzyme inhibitors, angiotensin-2 receptor blockers, phosphodiesterase 5 inhibitors)
- Non-steroidal anti-inflammatory drugs
Uncommon
Internal/external nasal valve incompetence
Neoplasm:
- Benign (eg haemangioma, papilloma)
- Malignant (eg nasopharyngeal carcinoma, squamous cell carcinoma, melanoma)
Empty nose syndrome – from previous excessive surgery
Trigeminal neuropathy
Rare
Anatomical
- Choanal atresia
- Pyriform aperture stenosis
Infective
- Human immunodeficiency virus
- Syphilis
Tuberculosis
|
History
When assessing a patient with nasal obstruction, the following factors should be considered:
- Is it unilateral or bilateral? Unilateral nasal obstruction suggests an anatomical cause. Bilateral non-dynamic obstruction may indicate an anatomical cause (eg nasal polyposis). Alternating nasal obstruction generally indicates mucosal inflammation manifesting in the normal nasal cycle.
- What is the timing? Are symptoms seasonal or diurnal?
- Are there specific triggers (eg exposure to smoke or pets)?
- Are there factors suggestive of infection? Purulent rhinorrhoea with facial pain and fever are seen in the case of acute sinusitis.
- Are there factors suggestive of neoplasia? Unilateral nasal obstruction with epistaxis raises the possibility of a neoplastic process. In this case it is important to enquire about ear symptoms as a postnasal space mass may impair Eustachian tube function and result in a unilateral middle ear effusion. Other factors suggestive of neoplasia, including malignancy, include paresthesia, diplopia and trismus, which are related to local extension of tumour into adjacent structures.
- Is there a medical history of atopy, asthma, aspirin sensitivity and co-existing inflammatory conditions?
- Is there a history of sinonasal surgery for septal deviation, nasal polyposis (risk of recurrence)4 or tumour?
- What medications are being used (Box 2)?4
- Is there a social history of note? Smoking can impair mucociliary clearance and is a risk factor for malignancy. Alcohol is a vasodilator and may cause mucosal congestion. A history of illicit drug use is important; for example, nasal administration of cocaine can lead to septal perforation. Exposure to hard wood dust (carpenters, wood turners) can predispose to sinonasal adenocarcinoma.
Examination
The examination should take into consideration airflow dynamics and areas where increased resistance can occur.5 A useful method is to commence with external examination of the nose followed by examination of the internal anatomy.
External examination should focus on deformities of the bony and cartilaginous structures of the nose, as well as the adjacent tissues. Examine for nasal tip ptosis and manually elevate the tip to a neutral position to assess for improved nasal obstruction. An improvement in air flow suggests an abnormality in the cartilaginous nasal tip.5,6 Examine the airflow during normal and deep inspiration, and assess for collapse of the nasal valve. The internal nasal valve provides the greatest resistance to airflow, hence even minor narrowing can cause nasal obstruction. Cottle’s manoeuvre (Figure 1B) can be used to assess if there is the cause of symptoms is related to this valve. In this manoeuvre, the cheek is held to prevent collapse of the nasal valve and the patient is asked to breathe through their nose to assess for improved flow. If this manoeuvre improves the patient’s symptoms, the cause is likely to be related to this valve.7
Anterior rhinoscopy of the nose requires a good headlight and a thudichum speculum.6 In the general practice setting the ‘pig nose’ manoeuvre (Figure 1C) is an alternative method where the patient’s head is tilted back, the nasal tip is elevated with the clinician’s thumb and a otoscope is used to illuminate the orifice. Examine the mucosal surfaces, the colour and calibre of the turbinates, and the position of the septum. Pale, boggy mucosa of the inferior turbinates is in keeping with rhinitis that is commonly of allergic aetiology. Red and oedematous mucosa is seen more commonly in infective or vasomotor rhinitis.5
If the diagnosis remains unclear the patient may need fibre optic nasal endoscopy in the specialist setting to examine the more posterior aspects of the nasal cavity.5 This is usually performed after the nasal cavity is prepared topically with a combination decongestant and local anaesthetic spray.
Finally, the patient’s neck should be examined for lymphadenopathy, and the ears for middle ear effusion, especially in those in whom sinonasal neoplasm is included in the differential diagnosis.6
The above history and examination will identify most causes of nasal obstruction; however, in patients in whom the cause is uncertain, the condition persists despite medical therapy, or where neoplasm is suspected, further investigation is warranted.

Figure 1. Nasal anatomy and clinically examination manoeuvres
A. A computed tomography scan of sinuses depicting important anatomical structures; B. Cottle’s manoeuvre: manually retract the cheek laterally and ask the patient to breathe through their nose to assess for improved flow. If this manoeuvre improves the patient’s symptoms, the cause is likely to be related to collapse of the nasal valve; C. The pig nose manoeuvre: the patient’s head is tilted back, the nasal tip is elevated with the clinician’s thumb and an otoscope is used to illuminate the orifice. This is particularly useful in children and in the general practice setting where a thudichum nasal speculum is not available
Imaging
Computed tomography (CT) is the preferred imaging modality for the nose and paranasal sinuses.8 In most cases, it allows for appropriate imaging of the sinuses and their drainage pathways and also investigates for extranasal extension of disease, such as into the orbit or intracranial cavity. Magnetic resonance imaging (MRI) is used when CT is inconclusive or where further characterisation of soft tissue or extranasal extension is required.9
Blood tests
If allergy is suspected, tests for allergen‑specific IgE (radioallergosorbent test) are commonly requested. Currently, the Medicare Benefits Schedule rebate for blood tests is limited to four tests at a time. Thus, dust mite mix, alternaria mould, grass pollen mix and animal dander mix may be appropriate. Food mix testing is common practice and false-positive results are commonly observed. Patients can continue antihistamines prior to these tests.6,10
Microbiology
If pus is seen, this can be swabbed to help guide antimicrobial therapy.6
Management
Management is focused on the underlying cause. If an anatomical abnormality is thought to be the cause, then management is largely surgical and referral to the otorhinolaryngologist for an opinion is required. First-line management for most causes of nasal obstruction is pharmacological and should be prescribed by the general practitioner. Some common aetiologies encountered are discussed below.
Allergic rhinitis
Intranasal steroids should be prescribed in those whose symptoms have an adverse impact on their quality of life.10 These agents are most effective if used regularly and accompanied by the use of a nasal douche, the intranasal steroid spray being used 15 minutes after the nasal douche. The nasal douche cleanses the nasal cavity of stagnant mucus, with the benefit of reducing the burden of allergen that is present in this mucus. Non-sedating antihistamines should also be prescribed for breakthrough symptoms, particularly sneezing and epiphora.10 If these treatments together with allergen avoidance are insufficient in controlling symptoms, then referral to an immunologist/allergist for immunotherapy should be considered.10 If inferior turbinate hypertrophy is also detected in the setting of failed conservative measures then referral to an otorhinolaryngologist for turbinate reduction may be indicated.10
Box 2. Treatments and medications commonly used in the management of nasal obstruction
|
Nasal douche
- Use four times a day during acute stage, can reduce to twice a day for maintenance
Saline nasal spray
Corticosteroid nasal sprays/drops:
- Beclomethasone 50 µg/dose, two sprays twice a day (S2)
- Budesonide 32 µg/dose (S2)
- Budesonide 64 µg/dose, one to two sprays in each nostril (S4)
- Ciclesonide 50 µg/dose 2 sprays in each nostril daily (S4)
- Fluticasone propionate 50 µg/dose, one spray in each nostril daily dose (S2)
- Fluticasone furoate 27.5 µg/dose, one spray in each nostril daily (S4)
- Mometasone 50 µg/dose, one sprays in each nostril daily (S2)
Antihistamine nasal spray
- Azelastine 125 µg/dose, one spray twice each day (S2)
- Levocabastine 0.5 mg/mL, two sprays in each nostril twice each day (S2)
Combination nasal spray
- Fluticasone propionate 50 µg/dose + azelastine 125 µg/dose (S4)
|
|
S2, schedule 2 (over the counter); S4, schedule 4 (prescription only)
|
Rhinosinusitis
Rhinosinusitis is managed by a combination of intranasal steroids and large volume (150 mL) saline rinse.11,12 Intranasal steroids are used to reduce all symptoms, improve the degree of nasal blockage and decrease the severity of rhinorrhoea.11 Saline irrigation two to four times a day should be prescribed and this helps rinse the sinuses and clear the nose of stagnant mucus.12 Antibiotics are an option when there is an infective component, but the type of antibiotic and duration of treatment are controversial. In the event of failed medical management for the appropriate duration of at least eight to 12 weeks, referral to an otolaryngologist is warranted for consideration of functional endoscopic sinus surgery.
Nasal polyposis
A short course of oral steroids (duration up to but not exceeding 21 days) results in an improvement in health-related quality of life and symptomatology.13 In clinical practice this should be combined with intranasal steroids and large volume saline rinse to assist in maintaining the reduced polyp size. Referral for polypectomy may be required if this fails.
Rhinitis medicamentosa
Where possible, the primary care physician should cease or substitute the agent felt to be responsible for this rhinitis.4 Overuse of over-the-counter decongestants is a common aetiology for this condition. For symptomatic relief, intranasal steroids may be considered.4 Agents that sensitise the nasal mucosa to cold air, including menthol and eucalyptus, may also provide symptomatic relief.
Conclusion
Both acute and chronic nasal obstruction are common presentations to the primary care physician. There are a number of aetiologies and most can be diagnosed and effectively treated at the primary care level. Clinical history and examination will often lead the practitioner to the most likely cause and help direct appropriate investigations and management. Referral to a specialist otolaryngologist may be required if the cause is anatomical or when symptoms are refractory to medical therapy.
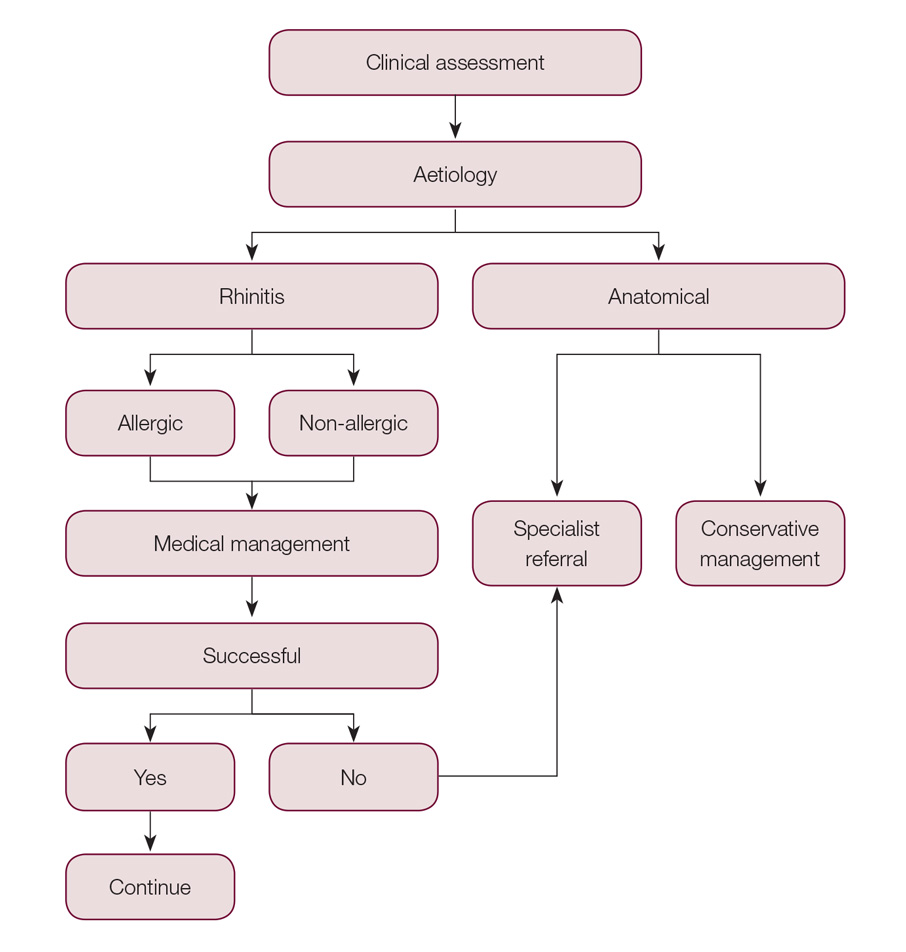
Figure 2. Clinical assessment flow chart
Case
A woman, 50 years of age, presents with a long history of nasal obstruction and rhinorrhoea. A history is taken according to the suggested protocol in this article. This reveals a chronic history of bilateral alternating nasal obstruction, right worse than left, with associated rhinorrhoea. The patient is a smoker and has a history of asthma.
On examination, the external nose appears normal. Anterior rhinoscopy by way of pig nose manoeuvre reveals septal deviation to the right and reactive hypertrophy of the left inferior turbinate. Cottle’s manoeuvre improves nasal airflow, particularly on the left side.
Management at this stage is to commence the patient on nasal douche four times a day and a corticosteroid nasal spray. A trial of three months is suggested, and if this adequately improve the patient’s symptoms, this treatment can be continued long term. If the patient’s symptoms are not adequately controlled, referral to an ear, nose and throat specialist may be required for consideration of septoplasty and turbinectomy.
Authors
Aaron Esmaili BPharm, MBBS (Hons), Service Registrar in Otorhinolaryngology, Head and Neck Surgery, Fiona Stanley Hospital, Murdoch and Royal Perth Hospital, Perth, WA
Aanand Acharya MBBS, MA (Cantab), MA, FRCS (ORL-HNS), FRACS (OHNS), Consultant in Otorhinolaryngology, Head and Neck Surgery, Fiona Stanley Hospital, Murdoch, WA; Royal Perth Hospital, Perth, WA; Saint John of God Hospital, Murdoch, Perth, WA; and Saint John of God Bunbury Hospital, Bunbury, WA
Competing interests: None.
Provenance and peer review: Not commissioned, externally peer reviewed.