Premature ejaculation is one of the most common sexual dysfunctions, affecting up to 21–31% of the Australian adult male population, irrespective of their age, marital status or ethnicity.1–5 This sexual condition is likely to be under-reported and under-treated because of the patients’ perceived shame and low self-esteem. This is in addition to many physicians feeling uncomfortable or uncertain about the management of premature ejaculation.6,7 The impact of premature ejaculation is mostly felt psychologically and in interpersonal relationships.8 Men with premature ejaculation often experience significant psychological distress, avoid physical and emotional intimacy, and become victims of false medical advertisings and unproven medical management.8–11
The aim of this article is to provide general practitioners (GPs) with an overview to assess and manage patients with premature ejaculation and other associated sexual dysfunction.
Definition and classification
Premature ejaculation is defined as the inability to control or delay ejaculation, which results in dissatisfaction or distress for the patient. Recently, the International Society of Sexual Medicine (ISSM) classified premature ejaculation as lifelong or acquired, and proposed inclusion of an objective, quantifiable time to ejaculation, which is referred to as the intravaginal ejaculatory latency time (IELT). The IELT is defined as the time from vaginal penetration to ejaculation. Lifelong premature ejaculation is characterised by an IELT of <1 minutes since first intercourse, whereas IELT of <3 minutes at any point in a man’s life is considered to be acquired premature ejaculation.12 Premature ejaculation can be further divided into authority-based subtypes ‘variable’ and ‘subjective’ (Table 1), which describe individuals experiencing significant distress and dissatisfaction with ejaculation.12
Table 1. Summary of the four classifications of premature ejaculation
|
|
|
Lifelong (primary)
|
Acquired (secondary)
|
Variable
|
Subjective
|
|---|
|
IELT criteria
|
<1 minute4
|
<3 minutes4
|
Short or normal
|
Normal or prolonged
|
|
Symptoms
|
Ejaculation occurs too early in nearly every sexual encounter
|
New onset of premature ejaculation, usually the result of an identifiable source and patient has experienced normal ejaculations in the past
|
PE is inconsistent and occurs irregularly and not the result of (psycho)pathology
|
Subjective, self- perception of rapid ejaculation despite normal ejaculation time
|
|
Onset
|
Early, usually from first sexual encounter
|
Can occur at any time in a man’s life
|
Can occur at any time in a man’s life
|
Can occur at any time in a man’s life
|
|
Prevalence
|
Low
|
Low
|
High
|
High
|
|
Quality of ejaculation control
|
Ejaculation remains rapid throughout lifetime with no ability to control ejaculation
|
Ability to delay ejaculation may be diminished or lacking
|
Ability to delay ejaculation may be diminished or lacking
|
Ability to delay ejaculation may be diminished or lacking
|
|
Aetiology
|
|
- Urological (erectile dysfunction, prostatitis)
- Hormonal (hyperthyroidism)
- Psychological
- Relationship problems
|
Normal variance of sexual performance
|
Psychological preoccupation with imagined rapid ejaculation
|
|
Treatment
|
- Pharmacotherapy
- Psychotherapy +/–
|
- Medical management
- Pharmacotherapy
- Psychotherapy
- Education
|
- Reassurance
- Education
- Behavioural therapy
|
- Psychotherapy
- Reassurance
- Education
|
|
IELT, intravaginal ejaculatory latency time
|
Pathophysiology and associations
Psychological components often contribute to acquired premature ejaculation. However, it is likely that a complex interplay between neurophysiological factors predominantly influence premature ejaculation. In particular, genetic predisposition for impairment of inhibitory serotonergic pathways that regulate ejaculation, modulated by 5-HT2c , 5-HT1a, 5-HT1b receptors and synaptic serotonin transporters has been reported for lifelong premature ejaculation.13,14 Other conditions, such as chronic prostatitis and hyperthyroidism, may also be associated with acquired premature ejaculation.15,16
Erectile dysfunction and premature ejaculation frequently co-exist,5,17 as men with erectile dysfunction might try to ejaculate early, before loss of erection.17,18 Thus, detection of comorbid erectile dysfunction is crucial in guiding therapeutic implementation.19
Assessment of premature ejaculation
Patients with premature ejaculation may present to general practice because of personal or partner-initiated reports of erectile or sexual dysfunction, and relationship difficulties. However, when the physician is unsure of the context of the presenting complaint, or uncertain about what to ask, an open-ended question, such as ‘How are things at home?’, may evoke disclosure of relevant symptoms. A full evaluation of the patient’s medical, sexual, psychological, social and drug history, along with his partner’s sexual history, is necessary to identify any factors that may be potentially reversible.
It is also important to explore the perceived degree of ejaculatory control, estimated IELT (precise timing is not necessary), previous attempts to correct premature ejaculation, and the impact on interpersonal relationships and quality of life. Various screening questionnaires such as the Premature Ejaculation Diagnostic Tool (PEDT), when combined with clinical assessment, are accurate in diagnosing premature ejaculation if it is unclear.20–22 It is particularly crucial to ascertain whether the diagnosis is lifelong or acquired, and be aware that erectile dysfunction may exacerbate the presentation. Simply inquiring about the loss of an erection before ejaculation can help to distinguish erectile dysfunction from premature ejaculation.
Physical examination of patients who experience premature ejaculation is often unremarkable. Full abdominal, neurological, lower limb and genital examinations are recommended. Although examination has a low diagnostic yield, it facilitates important reassurance for the patient that he is anatomically normal. There are no specific investigations to confirm or exclude premature ejaculation. Any additional investigations should investigate suspicion of contributory factors identified during history and examination.
Management of premature ejaculation
Ideally, discussions about management should involve the patient and his regular sexual partner. Treatment choice requires consideration of symptom severity, reversible causes, psychosocial impact, side effects and patient preferences.23
In clinical practice, management is complex and requires a combination of pharmacological, psychological and behavioural treatments (Figure 1).
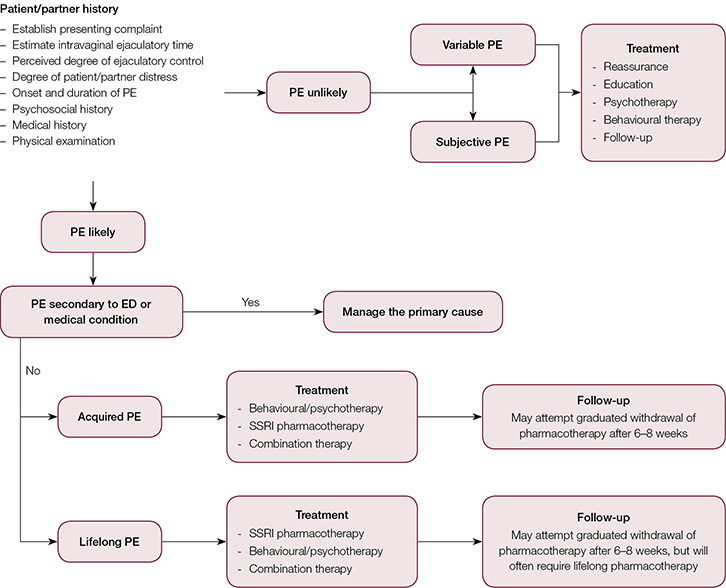 |
Figure 1. Premature ejaculation management algorithm4
Reproduced with permission from Althof SE, Abdo CH, Dean J, et al. International Society for Sexual Medicine’s guidelines for the diagnosis and treatment of premature ejaculation. J Sex Med 2010;7:2947–69. |
Conservative management options
Psychological therapy
Initially, psychological therapy was the mainstay of treatment for premature ejaculation. It is used less in current clinical practice because of time constraints, costs and requirement for strong compliance from couples.
Inconsistent, randomised evidence evaluating psychological therapy suggests its efficacy decreases over time24 and is inferior to pharmacotherapy.25 However, psychological therapy may be a suitable first-line treatment for patients with subjective premature ejaculation, or when a clear psychological aetiology is present.26 This can also be used to manage distress related to sexual dysfunctional, or in combination with pharmacotherapy.12,27
Behavioural therapy
Various behavioural changes have been suggested in the literature. For example, precoital masturbation is widely thought to improve IELT, but there is a lack of data to support this practice. Alternative behavioural therapy modalities attempt to attenuate the sensory responses of ejaculation by interrupting heightened arousal. These include the ‘stop-start’ (ceased genital stimulation until heightened arousal sensation subsides)28 and ‘squeeze’ (where the glans prepuce is squeezed at heightened arousal)29 techniques. These techniques are often considered intrusive, mechanical and disruptive of the normal spontaneity of coitus, and of little benefit when used alone. Other behavioural techniques include the use of multiple condoms and pelvic floor exercises. These techniques may improve premature ejaculation when combined with pharmacotherapy, but further efficacy studies are required.30
Complementary and alternative therapy
There is limited evidence supporting the use of acupuncture for the treatment of premature ejaculation.31 However, complementary and alternative medicine is not a recommended form of treatment for premature ejaculation.32
Medical management
Topical anaesthetic agents
Anaesthetic aerosols and creams containing lignocaine, lignocaine/prilocaine or herbal-derived anaesthetic agents can increase IELT and sexual satisfaction. These agents are often recommended as treatments for premature ejaculation.12,33–35 They are applied to the glans penis well ahead of sexual intercourse and should be used in conjunction with condoms to avoid numbness in the partner’s genitals.
Table 2. Summary of current medical agents for premature ejaculation
|
|
Agent
|
Recommended dose
|
Half-life (hours)
|
IELT fold increase
|
Adverse effects
|
Additional notes
|
|---|
|
Dapoxetine
(SSRI) – short acting
|
30–60 mg,
1–3 hours before intercourse
|
1.5
|
2.5–3
|
Nausea, diarrhoea, headache, somnolence, dizziness
|
- TGA approved, not currently on PBS
- No significant drug–drug interactions
- Effective treatment for both acquired and lifelong PE
|
|
Paroxetine
(SSRI)
|
10–40 mg/day and
20 mg, 3–4 hours
prior to intercourse
|
21
|
11.6
|
Insomnia, anxiety, nausea, loss of libido, ED, anhidrosis
|
- Off-label prescriptions
- Used for lifelong and acquired PE
- Therapeutic effect achieved in 2–3 weeks
- May hinder sperm motility
- May induce mania in bipolar patients
- On-demand use not as effective without daily regimen
|
|
Fluoxetine
(SSRI)
|
20–40 mg/day
|
36
|
5
|
Insomnia, anxiety, nausea, loss of libido, ED, anhidrosis
|
|
Sertraline
(SSRI)
|
50–200 mg/day and
50 mg, 4–8 hours prior to intercourse
|
26
|
5
|
Insomnia, anxiety, nausea, loss of libido, ED, anhidrosis
|
|
Clomipramine
(TCA)
|
12.5–50 mg/day and
25 mg, 4–24 hours prior to intercourse
|
19–37
|
6
|
Nausea, dry mouth, ED, hot flushes, arrhythmias
|
|
Tramadol
|
25–50 mg, 3–5 hours prior to intercourse
|
5–7
|
4–7.3
|
Nausea, dizziness, insomnia, dyspepsia, seizures
|
- Possible opioid addiction
- TCAs and SSRIs are contraindicated with Tramadol use
- Multiple drug interactions-only indicated as monotherapy in refractory PE
|
|
Phosphodiesterase-5 inhibitors
|
25–100 mg, 30–50 minutes
prior to intercourse
|
3–6
|
Monotherapy has no effect on IELT
|
Headache, flushing, dyspepsia
|
- Used for concomitant ED and PE
- Improved efficacy when combined with SSRI therapy
- Not established monotherapy for PE
|
|
Prilocaine-lignocaine topical cream/aerosols
|
2.5 g, applied 20–30 minutes prior to intercourse
|
1–2
|
4–6
|
ED, loss of sensation in penis and partner’s vagina, skin irritation
|
- Condom use encouraged
- Used with SSRIs
- Off-label prescription
|
|
ED, erectile dysfunction; SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressants; TGA, Therapeutic Goods Administration; PBS, Pharmaceutical Benefits Scheme
|
Serotonergic antidepressants
Serotonin inhibits ejaculation and its effects are potentiated by tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs). TCAs are effective, but infrequently used because they have prominent side effects, including nausea, dry mouth, erectile dysfunction, hot flushes and cardiotoxicity. Clomipramine is the only TCA in routine use.12,35
The therapeutic efficacy of SSRIs for premature ejaculation is well supported by the literature.36 Daily SSRI use may improve ejaculation delay after a few days; maximal delay is usually achieved after 1–2 weeks. Paroxetine is the most effective SSRI. However, paroxetine is not suitable for on-demand use because it has a slow onset of action (5 hours) and long half-life (1–3 days), and daily dosing is required to maintain efficacy.12 Daily SSRI dosing is more effective than on-demand treatment and is often favoured by patients because spontaneity of sex is maintained; however, compliance issues can occur with long-term use.
Doses of SSRI for premature ejaculation are significantly less than those used for depression, but have a similar side effect profile. Common side effects are fatigue, nausea, diarrhoea, dry mouth and decreased libido.37 There are also anecdotal accounts of infertility.38 Serotonin syndrome may also pose a risk if the patient is on concomitant treatment with drugs that elevate serotonin levels.37
Despite evidence supporting the use of clomipramine and traditional SSRIs (eg paroxetine, sertraline and fluoxetine) for the treatment of premature ejaculation, they are not licenced for treatment of this condition. As such, use of these agents for premature ejaculation would be off-label and incur costs to the patient, as they are not subsidised by the Pharmaceutical Benefits Scheme (PBS) for this indication.24
In 2010, the Therapeutic Goods Administration (TGA) approved dapoxetine for the use in premature ejaculation in Australia. However, this remains unsubsidised by the PBS. Dapoxetine is a newly developed SSRI that is rapidly absorbed (1–3 hours) and provides fast-acting treatment of premature ejaculation.39 Similarly to other SSRIs, dapoxetine should be used with caution in patients with cardiac, hepatic or renal impairment. Dapoxetine has been shown to increase IELT by 2.5–3 minutes with minimal adverse effects.36,40 Patients should take 30 mg of dapoxetine at least 30 minutes before sexual intercourse. Published studies found dapoxetine to be equally effective in men with lifelong and acquired premature ejaculation. It was also found to be well tolerated in men with premature ejaculation and comorbid erectile dysfunction treated with phosphodiesterase-5 type drugs.36,40
Phosphodiesterase-5 inhibitors
The precise beneficial mechanism of phosphodiesterase-5 inhibitors for premature ejaculation is unclear and its use as monotherapy is controversial.41,42 It does not affect IELT but may improve premature ejaculation in patients with comorbid erectile dysfunction by providing a perception of greater control over ejaculation.41 In this population, guidelines suggest treating erectile dysfunction and assessing the response on premature ejaculation symptomatology.12
Tramadol
Tramadol is an effective, on-demand treatment for premature ejaculation, although the mechanism of action is unknown. Doses of 25–62 mg were well tolerated, compared with placebo, and were found to significantly increase IELT, heighten sexual satisfaction and improve ejaculatory control.43,44 These results were more pronounced in patients with severe premature ejaculation (baseline IELT <1 minute). Tramadol has a number of drug interactions and should be used with caution in combination with SSRIs because of the risk of serotonin syndrome. It should only be considered for monotherapy use in men with refractory premature ejaculation.12 Ongoing studies are required to evaluate drug interactions, opioid dependence issues and the underlining mechanism of action.43
Surgical management
Circumcision and surgical management options for premature ejaculation are currently under investigation and not recommended. Experimental surgical therapies, such as dorsal penile nerve cryoablation, and neuromodulation and hyaluronic acid gel glans augmentation for refractory lifelong premature ejaculation have been reported to improve IELT.45–47 Botulinum toxin injections into ejaculatory muscles are currently being explored to prevent premature ejaculation.48
Follow-up and referral
Follow-up is an essential part of premature ejaculation management. It facilitates treatment optimisation, emphasis on key features of premature ejaculation and enables additional information gathering.49 In complex or refractory cases, specialist assistance may be sought from a sexual health physician or urologist. Input from sex therapists or psychiatrists may also be beneficial.
Conclusion
Premature ejaculation is the most common cause of male sexual dysfunction. Most patients who experience premature ejaculation are likely to require multi-modal management strategies involving pharmacological, behavioural and psychological components. Patients should be monitored closely to ensure treatment and sexual satisfaction.
Key points
- Premature ejaculation is the most common cause of sexual dysfunction, especially in the younger age group.
- It is estimated that premature ejaculation affects up to 31% of Australian males.
- Premature ejaculation causes significant psychological, emotional and interpersonal distress for the patient and his partner.
- Premature ejaculation can be lifelong (primary) or acquired (secondary), and this distinction guides management.
- Management of premature ejaculation should involve the patient and his partner, and is likely to require a multi-modal approach with pharmacological, behavioural and psychological therapies.
- Currently, no premature ejaculation therapies are subsidised by the PBS.
Authors
Eric Chung MBBS, FRACS, Consultant Urological Surgeon, University of Queensland, Princess Alexandra Hospital, Brisbane QLD; and AndroUrology Centre, Brisbane QLD. ericchg@hotmail.com
Brent Gilbert MBBS, Urology Resident Medical Officer, Mackay Base Hospital, Mackay QLD
Marlon Perera MBBS, Urology Registrar, Mackay Base Hospital, Mackay QLD
Matthew J Roberts MBBS, PhD, Urology Registrar, Mackay Base Hospital, Mackay QLD, and The University of Queensland, School of Medicine, Brisbane QLD
Competing interests: Eric Chung has previously been paid for consultancy and/or lectures by Lilly, GSK and Astellas.
Provenance and peer review: Not commissioned, externally peer reviewed.