In 1891, the University of Melbourne’s Clara Stone and Margaret Whyte joined the University of Adelaide’s Laura Fowler in becoming Australia’s first female medical graduates. Since then, the female presence has been instrumental in moulding the way medicine is practised.1,2 Women now make up over a third of the Australian medical workforce.3 In 1996, a prediction was made by the Australian Medical Workforce Advisory Committee (AMWAC) that women will make up 42% of the medical workforce by 2025.3 Indeed, 50.5% of commencing medical students and 65.8% of advanced vocational general practice registrars are female.4
Given these numbers, it would be reasonable to expect a strong influential female presence in medical decision-making circles with the ‘female voice’ heard across the spectrum of medical education, healthcare policy and clinical practice. Yet, in spite of the fact women have achieved leadership positions in a number of medical colleges over the past 20 years, and six of the current 17 professors of general practice are women, the female ‘voice’ is still struggling to be heard across the spectrum.3,5
The female voice or perspective in medicine refers to the incorporation of the female perspective in policy, planning, advocacy and politics.5–7 However, many of the medical meetings and medico-political forums occur after hours. Numerous studies and commentaries have found this can be problematic for women.5,6,8,9
Eighteen years ago, the AMWAC predicted that as the majority of female graduates were under 45 years of age, female-gendered work patterns would increasingly impact on workforce supply, including general practice.10 Since then, a multiplicity of studies have explored the experiences of ‘being a female practitioner’, dissected the working styles and patterns of men versus women, and looked at the gendered nature of the consultation.5,8,11–13 However, little work has explored why the increased presence of women in medicine has not mirrored an increase of the ‘female voice’ in the medical-leadership context, or what barriers to such an involvement might be.
Leadership requires multifactorial qualities, and medical leadership is no different.14 In 2010, the Academy of Medical Royal Colleges in the UK produced a 93-page document on the core competencies of shared medical leadership. These were identified as working with others, setting direction, demonstrating personal qualities, managing services and improving services. This is not necessarily a role-designated definition of leadership and allows all doctors to be potential leaders.15 Yet, Chadi focused on the importance of ‘having fully trained physicians occupying leadership roles relevant to the practice of medicine’.16 This study, therefore, includes a broad definition of leadership that encompasses a designated leadership role, as well as leadership competencies such as direction setting, which can exist without a designated role.
The aim of this article is to provide the findings of a small exploratory study, which sought to document female GPs’ participation in medical leadership roles and activities, and their perceived barriers to such involvement.
Method
This exploratory survey was distributed to a purposively-selected, convenience sample of 30 female general practitioners (GPs) in an inner eastern region of Melbourne, Australia. The survey period was for 3 weeks in February, 2012.
Survey instrument
The survey consisted of 20 questions listed in Appendix 1 (available online only). It was developed by one of the authors (KP), by drawing on her own experience and through consultation with colleagues. It was designed to collect perceptions and activities of female GPs in non-clinical medical leadership roles. There were a number of non-clinical roles, including in teaching, mentoring, medical politics, Medicare Local organisations, women’s professional groups, medical education, or business activities. A space was left for ‘other’ so participants could fill in freehand. The survey consisted of both open and closed questions, exploring issues including:
- participants’ attendance at non-clinical, medical meetings and/or activities previously listed
- participants’ level of involvement in these meetings and/or activities
- aspirations to increase their ‘leadership’ role in these meetings and/or activities.
Notably, the after-hours care component was included to provide a contrast as a medical activity compared to non-core clinical work of medical advocacy or leadership roles, particularly within general practice.
A specific definition of medical leadership was not provided to the participants. For the purpose of our study, ‘leadership’ was implied as holding any kind of post, position, or having a role that provided the ability to express leadership competency, thus setting the direction or activity of a group, committee or organisation. ‘Participation’ in an activity was implied, for the purposes of contrast, to be a passive, non-influential role.
Data management
All responses were entered into a Microsoft Excel spreadsheet and simple frequency statistics were used.
The survey was voluntary and anonymous, with participants unable to be retrospectively identified. A return-address envelope was supplied.
Ethics approval was granted by the Monash University Human Research Ethics Committee, satisfying section 5.1.22 of the National Statement on Ethical Conduct in Human Research (F14/1091-2014000470).
Findings
Twenty-five of the 30 GPs (83%) who were mailed the survey responded and their basic demographics are summarised in Table 1.
Notably, 88% of participants attended at least one medical-education meeting per month. However, question four of the survey asked the participants directly: ‘Do you ever feel inhibited in speaking at medical or political meetings?’.
Table 1. Demographics of participants
|
|
Participant characteristics
|
Percentage (n = 30)
|
|
Australian medical graduate
|
88
|
|
Married
|
84
|
|
Dependent children
|
68
|
|
Age (years)
|
|
|
20–29
|
8
|
|
30–39
|
28
|
|
40–49
|
28
|
|
50–59
|
28
|
|
60–69
|
4
|
|
70+
|
4
|
|
After-hours clinical care provided
|
24
|
|
Domestic labour involving 10–25 hours per week
|
60
|
Surprisingly, only 4% indicated they ‘never’ felt inhibited to speak at medical or political meetings, with 48% responding ‘sometimes’ and 48% ‘always’. Twenty percent of respondents held ‘leadership’ roles, and 12% were practice owners. This was in contrast with almost half the respondents (48%) having previously held ‘leadership’ positions at university, high school or other organisations.
Sixty percent of participants stated they felt they had support at home to pursue a leadership role. However, fewer women were currently in professional leadership roles, compared with participatory roles. Nor did these women aspire to increase their professional leadership roles in the future (Figure 1).
Medical mentoring was the most attractive future professional role for leadership aspirations. The least attractive option, for participation or leadership, was for medico-political organisations. The 30–39 age demographic had the greatest aspiration for leadership in this small sample, however, this virtually disappeared in the 40–49 age group.
A range of potential barriers to participation were identified by respondents in attending after-hours meetings or providing after-hours care (Figure 2), with ‘energy’ being the main participation barrier identified (60% and 48%, respectively). Energy for the purposes of this pilot survey was not quantified. Energy reflects the participants’ perception and could theoretically range from transient tiredness to burnout.17,18 Location of the meetings and after-hours care, and self-motivation ranked as second and third impediments, respectively.
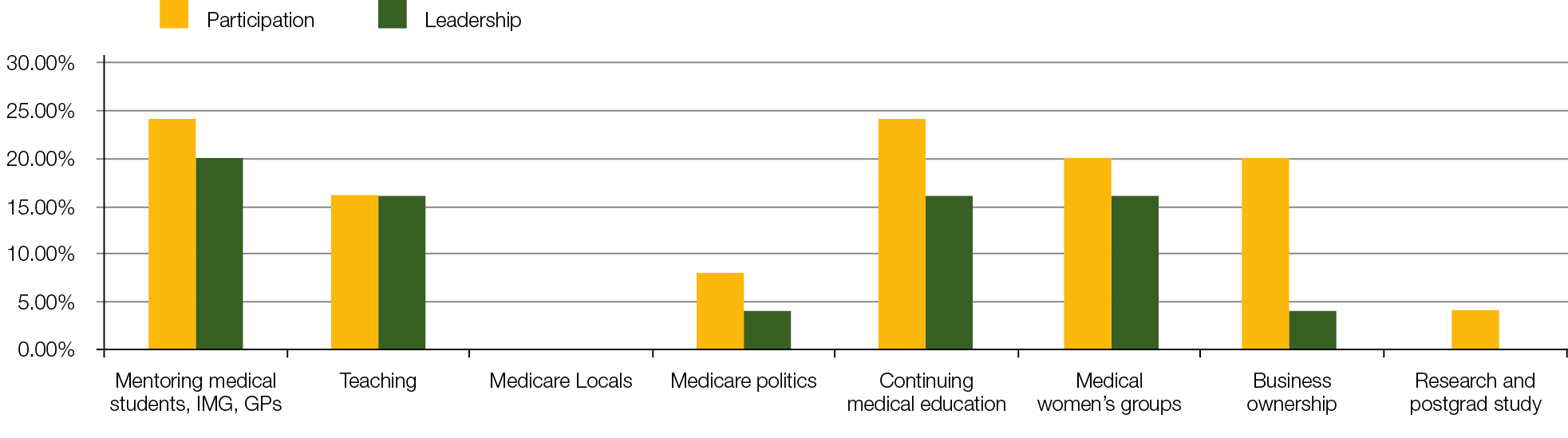 |
| Figure 1. Future aspirations for professional roles |
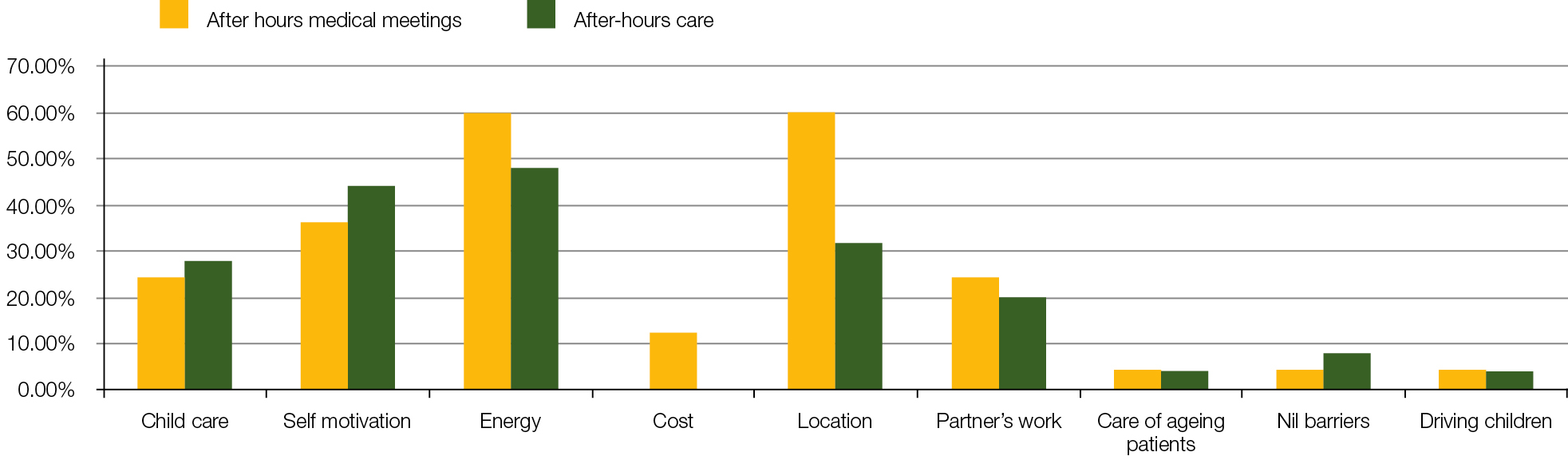 |
| Figure 2. Barriers to after-hours medical meetings or attending after-hours care |
Discussion
One of the findings of this investigation was the female GPs surveyed cited a lack of energy as a key barrier for their participation in after-hours activities. In addition, even when they did summon the energy to get to after-hours meetings, they often lacked confidence to speak up. From this small study, while women seek participation in after-hours activities, there may be inhibitions or barriers to them assuming leadership or input at these activities. Some have labelled this as ‘self-silencing’ and explained the phenomenon as a strategy to avoid crossing traditional gender stereotypes and experiencing negative evaluation from others.19 If this is the case, then Kilmartin’s suggestion that ‘women GPs need a stronger voice in decision making in the profession’ may still be some way off.8
This finding is also consistent with the prescient voice of Professor Carol Black and elucidated further by Professor Iona Heath in 2004, that the gender gap of experience, confidence, political interest, structural barriers and opportunity may render general practice, in particular, vulnerable and voiceless.9,20
This survey also highlights the relatively large amount of domestic work the participants were undertaking. Table 1 shows that 60% were performing 10–25 hours of domestic labour a week. Domestic labour referred to all unpaid domestic work being undertaken within the home, including housework and emotional ‘care’ work.21 It is not surprising, therefore, that for female GPs, energy levels rated highly as a barrier for after-hours meetings and the provision of after-hours general practice care. Literature suggests career aspirations are affected by gender and the perceptions that role conflict may contribute as a barrier to participation.22,23 The triple burdens of family, work and home life represent a potential role conflict for women that puts them at risk of burnout.24 This pilot is suggestive that issues relating to energy and domestic role conflict are still operating for these study participants.
Finally, another main barrier for participation in medical meetings mentioned in this study was the location of the meetings. In this regard, the internet and social media may be well positioned to facilitate female GPs’ involvement in after-hours meetings. The leadership role of mentoring, which was favoured by the women in this survey, may be useful to facilitate and develop female leaders as role models and promote female professional networks. Thus, professional skills and leadership development may be interesting to explore as a core requirement for all medical education bodies.
Limitations of the study
The outcomes from this small exploratory survey cannot be generalised due to the nature of the study and lack of formal validation of the survey instrument. However, the findings of a lack of energy and self-confidence as two major impediments to female GPs’ involvement in non-clinical professional roles warrants further exploration in a larger study that embraces the opinions of both men and women using a validated instrument.
Conclusion
As the number of women in medicine increases in all specialities, in particular general practice, it is important female and male perspectives are captured in health policy documents and the tenets of service delivery. Identifying barriers that may prevent this is an essential first step in exploring solutions. This small survey has suggested two factors that may be restricting women’s capacity to engage in leadership roles – energy limitations and lack of self-confidence. While the issues are complex and more research is required, the challenge is to frame these issues as opportunities to develop the profession, and maintain its professional integrity and professional independence. In that case, the gender of the practitioner becomes irrelevant, remaining mindful of Hilary Clinton’s 2011 Asia-Pacific Economic Cooperation (APEC) statement that ‘evidence of progress is not evidence of success’.25
Appendix 1. Demographics of participants
|
|
1. Please circle if you did graduate in Australia?
|
Yes
|
No
|
|
2. Regarding your household, are you the primary income earner? Please circle.
|
Yes
|
No
|
|
3. Please provide, by circling, a very brief self-description in general terms regarding your personality?
|
Introvert
|
Extrovert
|
|
4. Do you ever feel inhibited in speaking at medical or political meetings? Please circle.
|
Yes
|
No
|
|
5. Have you had any previous leadership experience during high school, university or other organisations? Please circle.
|
Yes
|
No
|
|
6. Do you already participate in leadership positions now? Please circle as you feel this applies.
|
Yes
|
No
|
|
7. Do you feel supported to pursue these roles? Please indicate by circling the most appropriate answer that applies to you now.
|
|
|
|
At work?
|
Yes
|
No
|
|
At home?
|
Yes
|
No
|
|
8. Thinking about the last twelve months, how many sessions do you work on average? Please circle.
|
0
|
1–4
|
|
9. Thinking about the last twelve months, can you estimate the total number of hours you spent on all home-based (non-medical) domestic work (not leisure) per week? Please circle the number of hours as indicated.
|
0
|
1–5
|
|
10. Please circle your age bracket in years as below.
|
20–29
|
30–39
|
|
11. Thinking about the last twelve months please circle the number of medical educational meetings you attend on average per month?
|
0
|
1–2
|
|
12. Thinking about the last twelve months and regarding your participation in any leisure activities, can please estimate the hours you attended these leisure activities outside of your work and home based work per week?
|
0
|
1–2
|
|
13. Do you have any dependent children?
|
Yes
|
No
|
|
14. Thinking about the last twelve months, do you provide after-hours care to patients (weeknights > 6.00 pm) or weekends? Please circle the number of hours if applicable per week.
|
0
|
1–2
|
|
15. What barriers, if any, do you perceive currently in attending after-hours meetings? Tick any of.
|
Childcare availability
|
Self-motivation
|
|
16. What barriers, if any, do you perceive in currently providing after-hours care? Tick any of.
|
Childcare availability
|
Self-motivation
|
|
17. Please circle your partnership status?
|
Single
|
Partnership
|
|
18. Other areas of participation (as opposed to leadership) you are interested in at any stage? Please tick any that apply or leave blank as applicable.
|
Mentoring medical students/IMG/general practice registrars/younger Drs
|
Teaching positions
|
|
19. Areas of leadership (rather than participation) you are interested in at any stage? Please tick any that apply or leave blank as applicable.
|
Mentoring medical students/IMG/general practice registrars/younger doctors
|
Teaching positions
|
|
20. Regarding your entire medical career, do you ever feel you have been discriminated against on the basis of your gender within the field of medicine?
|
Yes
|
No
|
|
Any comments relevant to any question:
|
|
|
Appendix 1. Demographics of participants
|
|
|
|
|
|
|
|
|
Sometimes
|
|
|
|
|
|
|
Other
|
|
|
|
|
|
|
Sometimes
|
|
|
|
|
|
|
Don’t know
|
|
|
|
|
|
|
Don’t know
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Don’t know
|
|
|
|
|
|
|
Don’t know
|
|
|
|
|
|
|
5–7
|
7–10
|
10+
|
|
|
|
|
6–15
|
16–20
|
21–25
|
25+
|
|
|
|
40-49
|
50–59
|
60–69
|
70+
|
|
|
|
3–4
|
5–6
|
6+
|
|
|
|
|
3–4
|
5–6
|
7–8
|
8+
|
|
|
|
|
|
|
|
|
|
|
3–4
|
5–6
|
7–8
|
8+
|
|
|
|
Energy levels
|
Cost
|
Location of meeting
|
Partners work
|
Looking after ageing parents
|
Nil barriers
|
|
Energy levels
|
Cost
|
Location of meeting
|
Partners work
|
Looking after ageing parents
|
Nil barriers
|
|
Separated
|
Other
|
|
|
|
|
|
Medicare Locals
|
Medico-political organisations
|
Continuing medical education
|
Medical women’s groups
|
Owning own practice
|
Other (specify)
|
|
Medicare Locals
|
Medico-political organisations
|
Continuing medical education
|
Medical women’s groups
|
Business partnership
|
Other (specify)
|
|
Don’t know
|
|
|
|
|
|
|
|
|
|
|
|
|
Competing interests: None.
Provenance and peer review: Not commissioned, externally peer reviewed.