Case
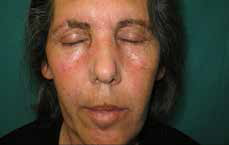
A woman, aged 72 years, living in a Spanish rural area, was referred to our dermatology department with a 10-month history of persistent, asymptomatic, brown, dirt-like facial macular dermatosis (Figure 1A). Her past medical history was unremarkable. Topical corticosteroids, topical fungal treatment (clotrimazole 1% cream) and scrubbing of the skin, including the use of soap and hot water, had been unsuccessfully tried. No complementary treatments were applied.

A |
B |
Figure 1
A. Persistent, asymptomatic, brown and dirt-like facial macular dermatosis;
B. Clinical image after firm rubbing with an isopropyl alcohol 70% swab |
Question 1
What is the diagnosis?
Question 2
How would you diagnose this disease?
Question 3
Given the clinical presentation, what other diseases should be considered?
Question 4
What are the treatment options?
Answer 1
Also called Duncan’s dirty dermatosis1, terra firma-forme dermatosis (TFFD) derives from Latin for ‘solid earth’ and is often suspected on the basis of its distinctive clinical presentation as hyperpigmented dirt-like brown patches and plaques. TFFD is not usually included in dermatology textbooks and only some case reports appear in the literature; hence, it is possible that it is often unrecognised or misdiagnosed. TFFD and dermatosis neglecta are widely considered to be synonymous but some authors have proposed a separation of both terms. TFFD occurs mainly in older children and adolescents with characteristic hygiene habits and with a distinctive distribution of the lesions, whereas dermatosis neglecta affects patients of any age whose hygiene in specific areas is insufficient.
Answer 2
Diagnosis is made mainly on the basis of clinical findings. Lesions may appear verrucous, reticulate and stuck-on, often affecting the neck, trunk and umbilicus. Most reports have described adolescents or young adults with a history of normal hygiene and vigorous but unsuccessful attempts at cleansing the affected areas.2 Swabbing firmly with 70% ethyl or isopropyl alcohol improves the appearance, confirming the diagnosis. In typical cases, histopathological examination is rarely necessary.
From the pathophysiological point of view it may be caused by a delay in the maturation of keratinocytes, with melanin retention and a sustained accumulation of sebum, sweat, corneocytes and microorganisms in regions in which hygiene measures are less rigorous.3
Answer 3
The differential diagnoses for TFFD include:
- acanthosis nigricans
- confluent and reticulate papillomatosis
- tinea versicolor
- ichthyosis vulgaris.
Other differential diagnoses to consider in the young population (2–14 years) are:
- post-inflammatory hyperpigmentation
- epidermal naevi
- atopic dermatitis.
Acanthosis nigricans (AN) typically presents with thickened, grey-brown hyperpigmented plaques on the skin. The back of the neck, sides of the neck and axillae are the most common sites of involvement. It typically develops in a symmetrical distribution and is usually asymptomatic. However, lesions in skin folds that become macerated and inflamed may become uncomfortable or malodorous.
Confluent and reticulate papillomatosis is a rare disease typically affecting young people (6–20 years). It is characterised by greyish blue hyperkeratotic papules usually located on the trunk. It may represent an endocrine disturbance, a disorder of keratinisation, an abnormal host reaction to fungi or bacteria, a hereditary disorder or a variant of amyloidosis. The eruption is chronic with exacerbations and remissions.
Pityriasis (tinea) versicolor is a superficial mycosis that occurs as many oval or round patches with mild scales. The most common colours are brown and tan. Seborrheic areas (upper trunk and shoulders) are the most commonly affected locations. The face may very rarely be affected.
Ichthyosis vulgaris is a skin disease that occurs in the first months of life. The lesions are usually thin pink or whitish scales located preferentially on the extremities. Groins and flexural areas are spared. Mild hyperkeratosis of palms and soles may be observed. In severe cases scaling extends to trunk, scalp, forehead and cheeks. Pruritus is an inconstant symptom.
The main clinical difference is that TFFD is typically associated with a velvety feeling surface.
Answer 4
This condition can be treated with the diagnostic method itself, that is, swabbing with 70% ethyl or isopropyl alcohol. It may also be treated with products such as salicylic-acid-based exfoliants or other keratolytic agents in order to accelerate the normalisation of the skin (ie 5% salicylic acid in sorbolene; 5–10% salicylic acid in vaseline; 17% lactic acid oil/water emulsion).4
The knowledge of this entity is important to avoid performing unnecessary skin biopsies and endocrinological evaluation to rule out insulin resistance.
Case continued
Firm rubbing with an isopropyl alcohol 70% swab immediately caused significant improvement of the skin condition (Figure 1B). The patient experienced no recurrence in the 12 months following treatment.
Key points
- TFFD presents as hyperpigmented dirt-like, velvety brown patches and plaques. It may be an under-recognised condition.
- TFFD typically occurs in areas of the body where hygiene measures have been not been rigorous.
- TFFD can be diagnosed and treated by swabbing with 70% ethyl or isopropyl alcohol.
- Recognition may prevent unnecessary investigations and inappropriate treatments.
Competing interests: None.
Provenance and peer review: Not commissioned, externally peer reviewed.