Control of blood pressure has been shown to delay or improve the outcome of a range of cardiovascular diseases (CVDs).1 People at high absolute CVD risk, which includes those who have already experienced a CVD event, have the most to gain from improved blood pressure control.2 A large, individual patient data meta-analysis concluded that lowering blood pressure provides progressively greater absolute CVD risk reduction as baseline risk increases,3 while the recently published SPRINT study4 has further shown the benefits of blood pressure control in people at high CVD risk.
In Australia, general practice is the key setting for interventions to improve the management of hypertension, as this is the context where hypertension is diagnosed and treated. Hypertension is the most common problem managed at general practice consultations, occurring at a rate of 9.1 problems per 100 encounters.5 However, blood pressure control, even in people at high absolute CVD risk, is often not optimal and many people with hypertension have behavioural risk factors for CVD. The AusDiab survey found that the prevalence of hypertension in the Australian population was 28.6%, with 13.4% treated with antihypertensive medicines.6 Of those on treatments, 60% had a blood pressure ≥140/90 mmHg, 20% were obese, 31% had diabetes, 29% had hyperlipidaemia, 27% were smoking, 23% had excessive alcohol intake and 28% had insufficient physical activity.6
The ImPress intervention is a systematic, population approach tailored to primary care. It is geared to identifying, recalling, assessing and treating patients with known hypertension who are at high absolute CVD risk and whose blood pressure is not treated to target. This intervention is novel as it targets nurse‑led care to those with the most to gain from improved blood pressure and control of other CVD risk factors. This complex intervention is based on the elements of the chronic care model,7 with a focus on clinical information systems, self‑management support and delivery system design.8,9 ImPress is primarily delivered by the general practice nurse (GPN) in collaboration with the patient and the general practitioner (GP). The Australian GPN workforce has grown exponentially, with most general practices now employing at least one registered nurse.10 The role of the GPN is well suited to guideline implementation, self‑management support and supporting behaviour change.11 This pilot study examined the impact of the ImPress intervention on blood pressure, anthropometric measures, treatment adherence and lifestyle behaviours. Qualitative feedback from GPNs, GPs and patients involved in the study is being reported separately.
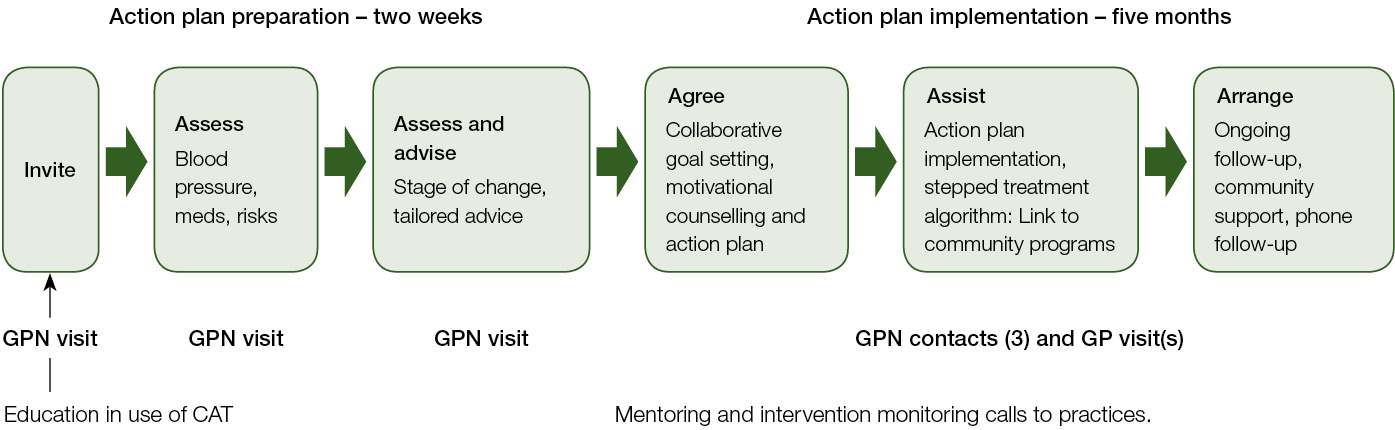
Figure 1. Impress intervention based on 5As framework
GP, general practitioner; GPN, general practice nurse
Methods
A before-and-after pilot study was conducted in general practices in metropolitan Sydney. Practices were selected for invitation to participate from the membership of the University of New South Wales (UNSW) practice-based research network (PHReNet–GP). Practices were eligible to participate if they used Best Practice or Medical Director software, employed a registered nurse, and both the nurse and GP were willing to participate in the study.
Potentially eligible patients were identified and invited to an assessment visit with the GPN via a search of practice desktop software using the Penn CS Clinical Audit Tool. Criteria for invitation were: aged 45–74 years; active patients according to The Royal Australian College of General Practitioners (RACGP) definition (ie attended three or more times in past two years); have a diagnosis of hypertension recorded; are at high risk of a CVD event (defined as five year absolute risk >15% or the presence of CVD); and have uncontrolled hypertension.
Uncontrolled hypertension was defined using criteria from the National Heart Foundation (NHF) of Australia’s hypertension guidelines1 as patients without an associated condition(s) or end-organ damage where their most recent manual office blood pressure measurement was ≥140/90 mmHg or, for those with an associated condition(s) or end-organ damage, the most recent blood pressure measurement was ≥130/80 mmHg. Letters of invitation were sent to these patients; non-responders had one follow-up phone call from the GPN.
Outcome measures were collected by the GPN at baseline and follow-up at six months. Physiological outcome measures were systolic and diastolic blood pressure (office measurement according to guidelines);1 body mass index (BMI), waist circumference, and waist-to-hip ratio. Treatment compliance measures were the Hill–Bone compliance to high blood pressure therapy scale12 and the Morisky medication adherence scale (MMAS-8).13
The Hill–Bone compliance to high blood pressure therapy scale assesses three behavioural domains of high blood pressure treatment: reduced sodium intake; appointment keeping; and medication-taking. This scale comprises 14 items in three subscales and is rated on a four-point Likert-type scale. The eight-item MMAS-8 has been used in hypertension and in a range of chronic illnesses. The first seven items are Yes/No responses, and the last item is a five-point Likert response. The additional items focus on medication-taking behaviours, especially related to underuse. Smoking, nutrition, alcohol and physical activity (SNAP)14 health behaviour measures were: self-reported smoking and alcohol use (based on questions from the New South Wales Health Adult Health Survey 2002 and Australian Bureau of Statistics National Health Survey 2001); dietary assessment (fruit and vegetable; cereal and cooked cereal; processed meat, hot and crisp chips; cereal and cooked cereal; type of milk consumed);15 and physical activity.16
Intervention
A one-day educational workshop was held for GPNs. This workshop covered the study rationale, study procedures, blood pressure measurement, use of study tools and collaborative care for hypertension management. GPNs were provided a template for a hypertension management action plan, which covered key issues in medicines adherence and lifestyle modification. Templates were also provided for the GPN assessment visit, each of the GPN face-to-face and telephone contacts and GP visits, as well as a tool for tracking patient progress throughout the intervention. All these were made available in an automatically pre-populating electronic format for use in both Best Practice and Medical Director software. The GPNs were also provided a stepped algorithm for treatment intensification from the NHF hypertension guide.1
Two weeks after the GPN workshop, a webinar was held with the nurses and participating GPs to explain the aims of the project to GPs, encourage commitment to participation, agree on roles and responsibilities, and discuss how progress of the intervention would be monitored in the practice. The intervention involved an assessment visit, development of the action plan and a series of contacts with the GPN and GP for implementation (Figure 1). The number of contacts was tailored to individual patients’ needs. Following the education workshops, the nurses were contacted by one of the investigators (EH) by telephone to provide mentoring and monitor implementation of the intervention.
Results
Practice recruitment for the study was rapid, with 13 practices, of 32 approached, responding; however, three practices withdrew before patient identification and invitation, and two further practices withdrew at a later stage, leaving eight practices that completed the project (Figure 2, flowchart for recruitment information and reasons for losses to follow-up). Thirteen GPNs (mean age 43 years) and 14 GPs (mean age 52 years) participated in the study.
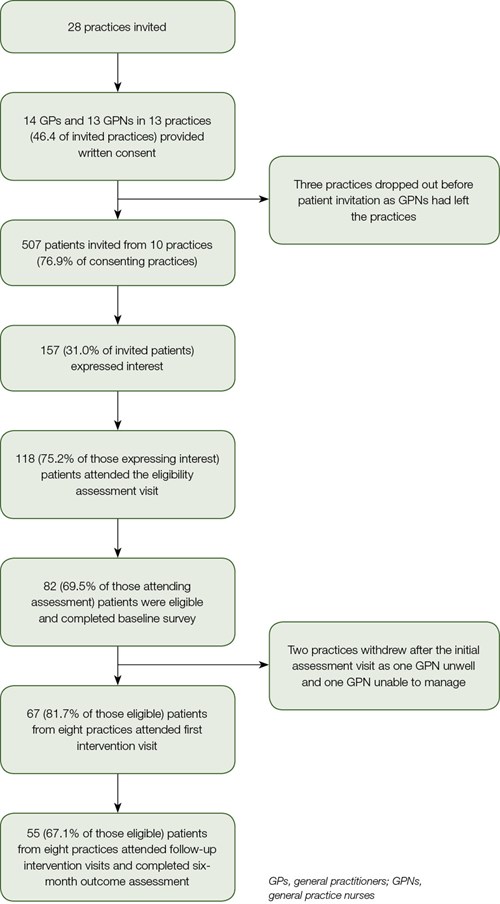
Figure 2. Practice and patient recruitment flowchart
The mean number of patients identified per practice with high CVD risk and uncontrolled blood pressure (based on the most recent blood pressure measurement) was 125. From the patients identified, a random sample of 507 patients was invited to attend the GPN assessment visit. Of these, 118 (23%) attended and 85 (72.0%) were confirmed as having uncontrolled hypertension. Of these, 82 patients consented to be involved and provided baseline data. The mean age of participating patients was 62.5 ± 19.2 years and 62.2% were male. Details of participating patients’ demographic characteristics are shown in Table 1.
Fifty-five patients (67.1%) provided follow-up data at six months. The mean decrease in systolic blood pressure was 14.5 mmHg (95% confidence intervals [CI]: –10.7, –18.2 mmHg) and diastolic 7 mmHg (95% CI: –4.3, –10.7 mmHg). Significant decreases were also found in mean weight (1.3 kg), waist circumference (1.9 cm) and BMI (0.6 kg/m2). Adherence to blood pressure treatment, as measured by the Hill–Bone scale, significantly improved (P = 0.01) and there was no significant change in medicines adherence as measured by the MMAS-8 (Table 2). No significant change was found in SNAP lifestyle behaviours, although there was a trend towards increased physical activity at follow-up (Table 3).
Table1. Patient demographics (n = 82)
|
Patient characteristic
|
Questions
|
|
|---|
|
Age
|
Mean (SD)
|
62.5 (19.2)
|
|
Sex
|
Male – n (%)
|
51 (62.2)
|
|
Female – n (%)
|
31 (37.8)
|
|
Married or de facto
|
Yes – n (%)
|
64 (78.0)
|
|
No – n (%)
|
18 (22.0)
|
|
Country of birth
|
Australia – n (%)
|
40 (48.8)
|
|
Other – n (%)
|
42 (51.2)
|
|
Language spoken at home
|
English – n (%)
|
58 (70.7)
|
|
Other – n (%)
|
24 (29/3)
|
|
Aboriginal or Torres Strait Islander*
|
Yes – n (%)
|
2 (2.4)
|
|
No – n (%)
|
50 (61.0)
|
|
Completed high school or higher
|
Yes – n (%)
|
57 (69.5)
|
|
No – n (%)
|
25 (30.5)
|
|
In paid employment
|
Yes – n (%)
|
26 (31.7)
|
|
No – n (%)
|
56 (68.3)
|
|
*Missing n (%) = 30 (36.6)
|
Table 2. Physiological and treatment adherence outcomes n = 55 unless otherwise stated
|
Variable
Mean value
|
Baseline
|
Six months
|
P value for difference in means*
|
|---|
|
Systolic blood pressure (mmHg)
|
149.2
|
134.7
|
<0.001
|
|
Diastolic blood pressure (mmHg)
|
88.1
|
80.6
|
<0.001
|
|
Weight (kg)
|
88.5
|
87.1
|
0.001
|
|
BMI (kg/m2)†
|
31.2
|
30.7
|
0.002
|
|
Waist circumference (cm)‡
|
106.0
|
104.2
|
0.034
|
|
Hip circumference (cm)§
|
109.8
|
108.5
|
0.131
|
|
Waist-to-hip ratio||
|
0.96
|
0.96
|
0.636
|
|
Morisky Medication Adherence Score (SD)#
|
2.02
|
1.75
|
0.240
|
|
(1.78)
|
(1.47)
|
|
|
Hill-Bone compliance scale (SD)**
|
19.8
|
18.9
|
0.01
|
|
(3.10)
|
(3.11)
|
|
|
*Paired sample t-test only includes cases that have values at both follow-up points †n = 50; ‡n = 54; §n = 51; ||n = 51; #n = 53; **n = 47; SD, standard deviation
|
Table 3. SNAP lifestyle behaviours
|
Variable
|
Baseline
|
Six months
|
P value for cross tabulation*
|
|---|
|
Non or former smokers†
|
48
|
48
|
0.56
|
|
≥5 serves of vegetables per day‡
|
5
|
7
|
0.67
|
|
≥2 serves of fruit per day§
|
29
|
27
|
0.82
|
|
Safe or no alcohol consumptionǁ
|
35
|
39
|
0.219
|
|
Adequate or high physical activity#
|
29
|
34
|
0.088
|
|
*Paired sample t-test only includes cases that have values at both follow-up points †n = 50; ‡n = 54; cn = 54; ǁn= 48; #n = 53
|
Discussion
The study found a substantial (14.5 mmHg, 95% CI: –10.7, –18.2 mmHg) reduction in mean systolic blood pressure from baseline to follow-up. This is larger than reported in a meta-analysis that found that nurse-led interventions, including a stepped treatment algorithm, reduced systolic blood pressure by a weighted mean difference of −8.2 mm Hg (95% CI: −11.5, −4.9).17 Our results are similar to the findings of a study conducted in Australian general practice, which examined the impact of a program of management with four GP visits and use of a stepwise drug titration algorithm.18 However, none of these studies was targeted to patients at high CVD risk, which is a novel aspect of our approach. Our results suggest that the likely mechanism of the effect is increased adherence to blood pressure treatment. This interpretation is supported by the improvement in adherence to blood pressure treatment as measured by the Hill−Bone scale. There was also a non‑significant improvement in the MMAS-8. However, there could be a range of other explanations for the change in blood pressure, including weight loss.1 It is also possible that a non-specific (Hawthorne) effect related to receiving an intervention and/or regression to the mean could account for some or all of the fall in blood pressure observed. How the weight loss and decreased waist circumference were achieved is not clear from our results as there was no significant change observed in dietary behaviours or in the level of physical activity.
Limitations
The major limitation of the study is the uncontrolled before-and-after design. The lack of a control group means we cannot be sure that the observed effects are due to the ImPress intervention rather than some other factor(s). There are also questions about generalisability, given that it was a small sample of research‑active practices that may be more enthusiastic to adopt innovations than general practices as a whole.
The PEN CS search and categorisation of target blood pressure is dependent on information on associated conditions and end-organ damage being accurately recorded in the diagnosis or reason for consultation fields of the electronic clinical record. This may not have been the case for all participants, so there may have been misclassification of target blood pressure levels for some patients.
The identification of uncontrolled blood pressure was on the basis of the most recent measurement and may have identified some patients whose mean blood pressure was within the target range.
The response to the invitation was 23% and there is a potential bias towards participation by more motivated patients. It should be noted that a response rate of approximately 20% is similar to that found in a previous study of a mailed invitation for a GPN intervention.19 Further research is needed to identify strategies to increase uptake of proactive care in general practice. There is also a risk of bias in the results due to loss of practices and, therefore, patients to follow-up.
Implications for general practice
The promising findings from this pilot study of the ImPress intervention, together with the positive feedback from GPs, GPNs and patients (authors’ own), justify further research in the form of a randomised trial. If effective, the approach would have major significance for how hypertension care is organised and delivered in Australian general practice and would support the implementation of evidence-based clinical practice guidelines. The model could potentially be implemented at scale with support from Primary Health Networks and be financially sustainable under the existing Practice Nurse Incentive Program. The approach of active practice population management is also relevant and transferable to other chronic conditions. Moreover, internationally, as there is an increased emphasis on primary care and population health approaches, the ImPress model of intervention shows promise.
Authors
Nicholas Zwar MBBS, MPH, PhD, FRACGP, Professor of General Practice, School of Public Health and Community Medicine, UNSW; School of Medicine, University of Wollongong, NSW. n.zwar@unsw.edu.au
Oshana Hermiz MBBS, Project Office, Centre for Primary Health Care and Equity, UNSW, NSW
Elizabeth Halcomb RN, BN (Hons), PhD, FRCNA, School of Nursing, University of Wollongong
Patricia Davidson RN, BA, Med, PhD, Dean, School of Nursing, Johns Hopkins University, Baltimore, USA
Thomas Bodenheimer MD, Professor, Department of Family and Community Medicine, University of California, San Francisco, USA
Competing interests: None.
Provenance and peer review: Not commissioned, externally peer reviewed.
Acknowledgements
We thank the patients, nurses and GPs who took part in this project. Funding was from a National Heart Foundation of Australia Vanguard Grant (award number 100246).