Although access to a wide range of contraceptive methods has improved over the past 30 years, appropriate use of these in the prevention of unintended pregnancy remains an issue of considerable health importance.1 Among women who continue their pregnancy, it has been shown that unplanned pregnancies are associated with higher rates of adverse infant and maternal outcomes,2 affecting women’s economic, psychological, physical, and social wellbeing.3 More than 70% of Australian women aged 16–50 years report using contraception,4 yet more than 50% of unplanned pregnancies in Australia occur in women using contraception at the time.5 These high rates of contraceptive use, and generally good access to services, suggest that most unplanned pregnancies in Australia are likely to be due to inconsistent use or failure of methods being used.1
The most commonly used contraceptive method in Australia is the combined oral contraceptive pill (COCP).1 Because the COCP relies on daily compliance, failure rates are often due to incorrect or inconsistent use.6 Conversely, long-acting reversible contraceptives (LARCs), including subdermal implants and intrauterine contraceptive devices (IUCDs), have very low failure rates because they are not user-dependent.6 There is some evidence for the potential of these methods to reduce rates of unintended pregnancy.4 Mavranezouli et al7 have reported that in the UK, if 5% of women who use the COCP as ‘typical’ users were instead to use a LARC method, decreased contraception failure would result in 7500 fewer unplanned pregnancies every year. Given the efficacy of LARCs, evidence‑based guidelines now recommend that these methods should be the first-line contraception offered to all women, including nulliparous and adolescent women.8,9 Not only do LARCs have a proven record of very high effectiveness, they are suitable for a wide range of women, and have been found to have very high user satisfaction.10 Increasing the use of LARCs could decrease unintended adolescent pregnancy rates, thereby improving maternal and infant health outcomes.10 Sexual Health and Family Planning Australia has advocated the need for further research into both facilitators and barriers of LARC uptake in Australia.11 Given the lack of previous in-depth research into IUCDs, we have decided to focus on this method alone.
Despite evidence of the advantages of LARCs, IUCDs are infrequently prescribed in Australia.12 Worldwide, 14.3% of women of reproductive age use IUCDs with rates as high as 40% in some regions, such as Central Asia. By contrast, in Australia, the use is negligible at 1.3%.12 The uptake of IUCDs depends on the healthcare providers who offer contraceptive counselling and are also responsible for insertion and removal of these devices.12 Research suggests that if more young women could access this method of contraception, there would be a greater uptake.13
Key stakeholders in the prevention of unintended pregnancies are doctors, especially general practitioners (GPs), who in Australia see 85% of the population each year.4 GPs hence play a critical role in prescribing IUCDs by providing correct information and following current guidelines when offering this method of contraception.9 Although most women access contraceptive services via their GP,14 no studies have explored barriers specifically faced by Australian GPs in prescribing IUCDs.
The aim of this study was to investigate perceived barriers faced by Australian GPs in the prescription of IUCDs, including counselling and insertion; and their views of the uptake of this method, particularly in young and nulliparous women.
Methods
A qualitative study design was selected to provide a detailed understanding of the knowledge and practices of participants. Semi-structured interviews, conducted in February–May 2016, allowed GP participants to discuss their perceived barriers, while also allowing key issues of the researchers to be explored.
Recruitment
Maximum variation purposive sampling was undertaken to explore potential differences among a diverse range of GPs. A matrix was developed for recruitment to ensure a combination of males and females, those practising in rural and urban settings, years since training, as well as inserters, non-inserters and previous inserters of IUCDs.
Participants were invited via VicReN (Victorian Primary Care Practice-Based Research Network), a collaboration between the University of Melbourne and more than 200 primary care practices around Victoria. Snowball sampling was used to ensure the sampling matrix was populated. The researchers had no prior relationship with any of the study participants before study commencement.
Data collection and analysis
Following collection of demographic data from participants, exploring their reproductive health practices, participants were interviewed using a pilot-tested schedule. This included questions of knowledge, attitude and practice around IUCDs.
All interviews were audio-recorded, and transcripts of the interviews were coded in NVivo and analysed using a conventional content analysis approach. Coding commenced after three interviews to aid in determining when data saturation was achieved. An iterative coding and analytical process took place, allowing the interviewer to include issues raised in subsequent interviews. A broad coding framework used the main categories within the interview schedule. After multiple readings of the transcripts, this coding framework was refined and data were grouped together into initial themes that emerged, with repeated reference to the transcripts. The research group reached consensus on key themes. All transcripts were re-read multiple times in light of these identified themes. Field notes taken after each interview were reviewed at the time of thematic analysis to confirm interpretation of themes.
Ethics approval for this study was granted by the General Practice Human Ethics Advisory Group, Victoria, Australia (application number 1545630).
Results
Participant characteristics
Overall, 17 interviews were conducted with GPs in Victoria, Australia, representing 16 distinct practice sites. Although data saturation was reached after nine interviews, a further eight interviews were conducted to seek a greater diversity of views.
Demographic details of participants are shown in Table 1. Two participants currently insert IUCDs, and five have been previous IUCD inserters.
Results were analysed manually by gender and rurality of participants; however, no significant differences in responses were found.
Table 1. Demographics of participating GPs
|
Characteristic
|
n = 17
|
|---|
|
Sex
|
|
|
Female
|
12
|
|
Male
|
5
|
|
Age (years)
|
|
|
25–34
|
3
|
|
35–44
|
5
|
|
45–54
|
2
|
|
55–64
|
5
|
|
≥65
|
2
|
|
Recruitment site
|
|
|
Urban
|
12
|
|
Rural
|
5
|
|
Employment status
|
|
|
Full time
|
7
|
|
Part time
|
10
|
|
Location where GP training was completed
|
|
|
Australia (urban)
|
7
|
|
Australia (rural)
|
6
|
|
UK
|
4
|
|
Other
|
0
|
|
Extra training relevant to women’s/sexual health
|
n = 22 (some participants had multiple certificates)
|
|
Diploma of Obstetrics
|
5
|
|
Family Planning Certificate
|
6
|
|
Other (including international certificates)
|
5
|
|
None
|
6
|
Analysis of interviews
All participants identified multiple barriers to IUCD access and uptake, from the perspective of patients and the practitioners.
Three main themes and eight subthemes emerged from this analysis:
1. Misconceptions brought to the consultation
1.1 Patients’ perspectives (perceived by GPs)
1.2 GPs’ perspectives
2. Lack of GPs currently performing insertions
2.1 Lack of training
2.2 Cost barrier: training and Medicare Benefits Schedule (MBS) rebates
2.3 De-skilling of previous inserters
3. Issues involved in the referral of patients for insertion
3.1 Time barrier
3.2 Cost barrier
3.3 Convenience of COCP
A broader overview of all barriers that emerged from the data analysis is detailed in Figure 1.
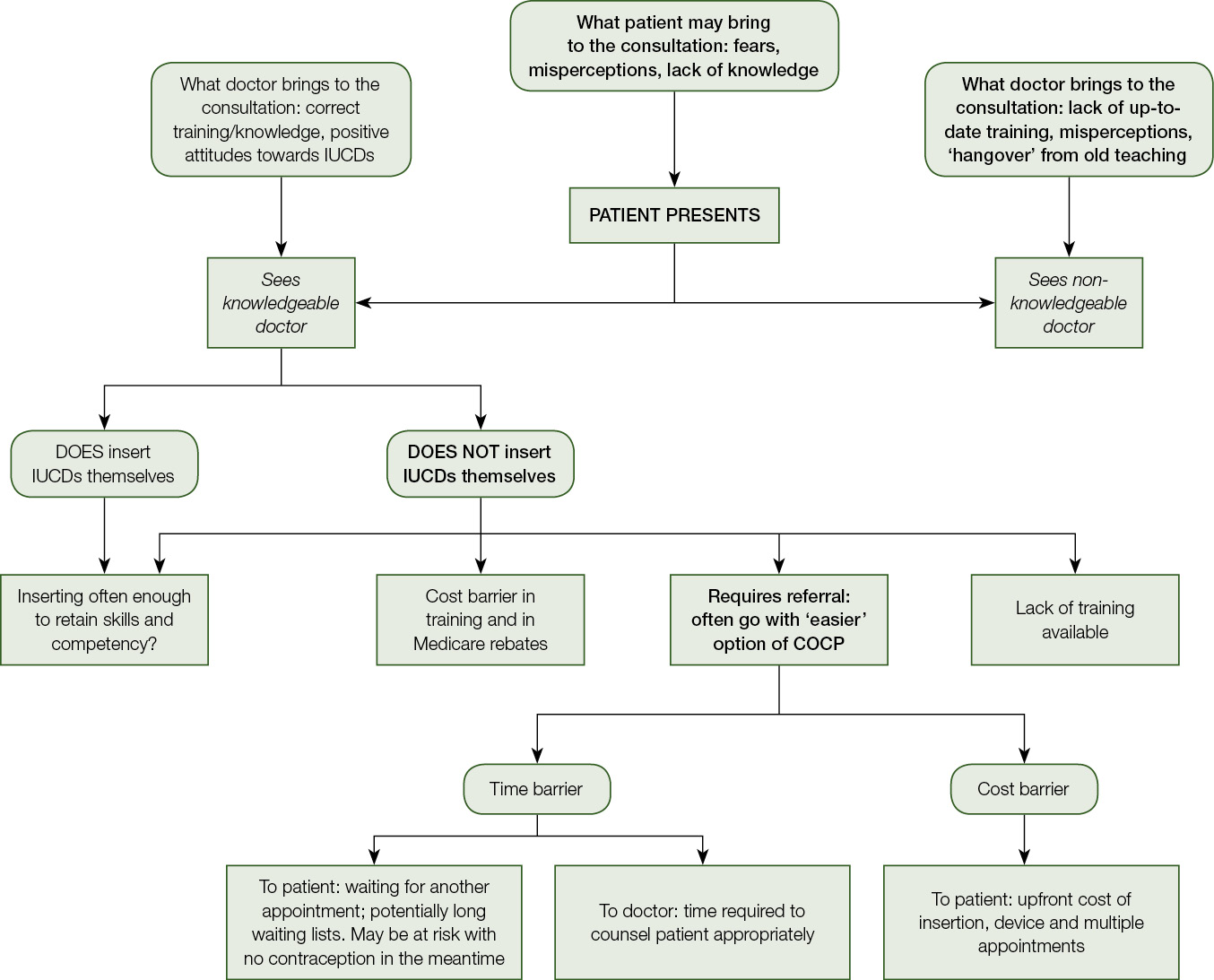
Figure 1. Overview of themes that emerged from data landscape
1. Misconceptions brought to the consultation
1.1 Patients’ perspectives (perceived by GPs)
Participants observed that many young women were unable to make informed choices about contraception because of limited knowledge or lack of knowledge about IUCDs.
Ignorance is probably the biggest barrier … the challenge is to make sure they have enough information to make an informed choice. − Male, age 58 years
Women just don’t know about them. They don’t seem to be publicised or talked about. − Female, age 58 years
Patients’ misconceptions of IUCDs were frequently implicated as a key barrier to the uptake of IUCDs, in particular, fears of the pain and invasiveness of the insertion.
They’re afraid of pain, afraid of side effects, afraid that it will be a traumatic experience getting it. − Female, age 29 years
I think there is still a perception by women that an IUCD is more invasive with lots of complications. − Male, age 64 years
GPs noted that young women had expressed fears of having a foreign body inside them, and this was a particular limitation to IUCD use.
As far as getting women to accept them, it’s partly around that idea of a foreign body that people don’t like. − Female, age 65 years
There is just the icky factor, some people don’t like the idea of having a foreign body inserted into them. − Female, age 51 years
1.2 GPs’ perspectives
Some GPs had expressed a very limited awareness and knowledge about up-to‑date guidelines for IUCDs, mainly in regards to patient eligibility. The ‘hangover’ from outdated teaching and knowledge was emphasised.
Doctors are lacking in education, and there is still a hangover from the days where you only put them in women who have had pregnancies, and you don’t put them in young women. − Female, age 61 years
There was still a bit of a hangover effect of the poor reputation of IUCDs, and so I can’t remember it being promoted necessarily as a good form of contraception. − Female, age 44 years
Some non-inserters had particular reservations in regards to the difficulty and pain believed to occur with insertion of an IUCD in a nulliparous woman.
I think the only thing with nullips is that technically it’s often trickier to insert. − Female, age 50 years
This was, however, strongly refuted by experienced IUCD inserters, who did not find this to be an issue, believing insertions to actually be easier in this population of women.
I actually find it easier to put it in younger women, in women who have not had pregnancies, because their cervix is not scarred, and it’s quite an easy procedure. − Female, age 58 years
Because of these misconceptions having a strong impact on practice, IUCDs are often not considered as an option for young and nulliparous women.
We were very definitely taught that IUDs are for multiparous women, women who are monogamous. −Female, age 51 years
I certainly wouldn’t encourage young women and nulliparous women to consider IUCDs. − Female, age 42 years
Despite this, some GPs had very positive attitudes towards IUCDs for all women, and were up-to-date in their knowledge of IUCDs.
I think they’re unbelievably effective contraception, really quite safe and well tolerated for most women. − Female, age 30 years
I’m not averse to recommending it or raising it as a possible option for younger women. − Female, age 50 years
2. Lack of GPs performing insertions
A major barrier to IUCD use, emphasised by some participants, was the large number of GPs who currently are not performing IUCD insertions.
More GPs inserting them is really the only solution to the problem of access. − Female, age 42 years
2.1 Lack of training
The current lack of training available for GPs to do insertions was highlighted as a major limitation.
We need to train more doctors to insert. − Female, age 58 years
There is inadequate training as part of GP and medical training. − Female, age 29 years
2.2 Cost barrier: Training and MBS rebates
A number of cost barriers to the GP undertaking training and performing insertions was emphasised. This included the cost of the actual training, as well as the unpaid hours required as part of this training.
The training course here is quite expensive. − Female, age 36 years
I have to take time off seeing patients to [get trained], and that is a financial cost … So there is no financial incentive for me at all to do it. − Female, age 35 years
Another aspect of concern around cost was the inadequate MBS rebate GPs receive to perform insertions.
I don’t think you get paid enough to put in an IUD from the MBS point of view. − Female, age 58 years
The big barrier is that it doesn’t pay…the rebate issue is a real issue for GPs. − Female, age 66 years
2.3 De-skilling of previous inserters
GPs who had previously performed IUCD insertions identified a further key barrier, which resulted in them no longer undertaking insertions. Some participants felt they were not inserting often enough to retain their skills, because of low patient demand.
I wasn’t doing enough to keep my skill set up I decided … you just become de-skilled. − Male, age 55 years
Because I have not been doing them, you get de-skilled. I wouldn’t feel comfortable putting one in at the moment. − Female, age 36 years
3. Issues involved in the referral of patients for IUCD insertion
When the GP could not insert the IUCD themselves, a range of access barriers, associated with the referral required for insertion, were raised. Limitations faced by doctors and the patients in this referral process were highlighted.
The more difficult you make it for someone to access a particular service, the less likely they are to actually do something. − Male, age 58 years
3.1 Time barrier
Participants indicated that the time required in sending women off to extra appointments, potentially associated with lengthy waiting lists, was a particular barrier to IUCD uptake.
Going down the IUCD pathway means sending someone to see the gynaecologist or to the family planning clinic, which is an extra step for the patient. − Male, age 33 years
Of particular concern to most of the GPs was that their patients are potentially at risk of an unplanned pregnancy if they have no contraception if there is a time delay for referral.
Referring them can be a five-month wait, and I don’t like the idea of younger women not having contraception for five months. − Female, age 61 years
If they are waiting to get it from the public service, they then may not be using any reliable or effective contraception in the meantime, and they are very much at risk of unplanned pregnancy. − Male, age 58 years
3.2 Cost barrier
The upfront costs for the patient, associated with the extra referral step and extra appointments, was another barrier to the uptake of IUCDs.
Seeing the doctor for the initial consultation, and then the insertion, and then the follow up, might mean that they can’t afford it, which would be a shame. − Female, age 30 years
That initial outlay can be a hindrance for some women, especially young women.− Female, age 44 years
3.3 Convenience of COCP
The interviews particularly highlighted the fact that GPs often find it easier to just prescribe the COCP instead of going through the referral process associated with an IUCD insertion.
It is more convenient just to come in and get a prescription of the pill.
− Male, age 55 years
It is easier to prescribe the pill. People can just say ‘here you are, here’s a prescription, now go away’. − Female, age 58 years
Discussion
Our study of Victorian GPs gave important insights into limitations in the prescription of IUCDs, and consequently in the uptake of this effective method of contraception.
Preconceived attitudes towards IUCDs were common misconceptions brought to the consultation by both the patient and doctor, and had an impact on the uptake of this method of contraception. It was promising that some GPs showed an interest in further education and updated training. Overall, these findings are consistent with international literature that has reported that clinicians’ misconceptions about IUCD appropriateness are major barriers to usage.9,14–21 As patients have an impact on driving the demand for contraception options, overcoming their misconceptions, a barrier that has been consistently recognised in similar work, must also be addressed.13,21–24
The lack of GPs who currently perform IUCD insertions was seen as an additional barrier. Major limitations to this were the lack of training available, the cost of being trained, and insufficient remuneration for the insertion procedure. The MBS rebate for the procedure currently sits at only $53.55, which is low when considering the time and skill for the procedure. It is also low when compared with Implanon insertion at $35.60, training for which is freely available.25 This barrier has not previously been reported as a concern for Australian GPs, probably because there has not been a qualitative study exploring GPs’ views on this issue.
For GPs not performing IUCD insertions themselves, barriers associated with the referral process presented a major limitation for uptake. To increase access to IUCDs, the time and cost barriers associated with these referrals would need to be minimised or removed.
Strengths and limitations
As Australian GPs have previously been reported as being the gatekeepers to women’s access to contraception,16 a strength of this study has been the ability to offer insight into GPs’ perspectives on prescribing IUCDs. However, despite efforts to minimise social desirability bias, participants knew that the interviewer had an interest in increasing IUCD uptake, which may have potentially resulted in an overestimation of IUCD counselling. A further limitation was the inability to directly interview patients, as this was outside the scope of the study. While recruited from a large network of Victorian GPs involved in teaching and research, these findings are from a purposive sample. In keeping with all qualitative research, the findings are not intended to be representative of all Victorian GPs, but to provide insight into perspectives which should be included in future quantitative research on this topic.
Implications for general practice
This research has highlighted potential causes for low prescription of IUCDs from the GPs’ perspective, which have been summarised in a conceptual framework presented in Figure 1. Each of the highlighted areas of patient factors, doctor factors, availability of GP inserters, and referral for insertion, contain key barriers. Targeting these areas may increase the access to, and uptake of, IUCDs.
If patients’ and doctors’ misconceptions of using IUCDs were overcome, it might be expected that women would make more informed choices about their contraception, which may increase demand for IUCDs. For women, ways of addressing patients’ misunderstandings could be via targeted social media campaigns, GP waiting room information, and school contraceptive programs. Further education of GPs about the advantages of IUCDs, and current guidelines recommending them as a first-line contraceptive option for all women,8,9 is likely to influence contraceptive counselling and prescribing behaviours.
To increase the number of GPs who can perform insertions with confidence and competence, structural barriers identified in this study would need to be addressed. Reducing current barriers to accessing training is critical, but the results of this study suggest that IUCD insertions would also need to be a cost-effective option for doctors. Increasing MBS rebates for IUCD insertions would increase the incentive for GPs to perform insertions, and would perhaps reduce the upfront cost for patients.
Rather than referring patients for IUCD insertion, increasing patients’ access to GPs who currently perform insertions has the potential to reduce costs and waiting times for patients, while maintaining the skills and competence of current GP inserters, due to greater patient volume.
The Australian government’s National Commission of Audit has shown that shifting provision of care into the lower cost primary-care setting, where clinically appropriate, will improve the efficiency of the health sector.26 Ultimately, increasing access to IUCDs in the primary-care setting will improve the likelihood that women are able to select the most effective contraceptive method for them, thereby helping to reduce the burden of unplanned pregnancies in Australia.
Conclusion
This study has identified numerous barrier faced by Australian GPs, from the GPs’ perspective, to the prescription of IUCDs. These include both the practitioner and patient’s knowledge and beliefs, the lack of GPs currently equipped to perform insertions, and concerns for patients created by access barriers to referrals for insertion. To further elucidate the extent of the issues highlighted in this study, future quantitative research on Australian GPs’ perspectives will be necessary. Future research is also required to explore Australian women’s views on IUCD use. However, the barriers to prescribing highlighted by GPs in this study indicate that there are challenges for women to access the full range of contraceptive options, potentially putting them at risk of unplanned pregnancies through the use of unreliable contraceptive methods. As unplanned pregnancies are associated with higher rates of adverse maternal and infant outcomes,2 contraception with a low failure rate is a substantial issue that should be easily managed in primary care.
Author
Gabrielle Lodge BBMED, MD, Melbourne Medical School, University of Melbourne, Parkville, Vic. gabbie.lodge@gmail.com
Lena Sanci MBBS, PhD, FRACGP, Deputy Head, Department of General Practice, Melbourne Medical School, University of Melbourne, Parkville, Vic
Meredith Temple-Smith BSc, MPH, DHSc, Director of Research Training, Department of General Practice, Melbourne Medical School, University of Melbourne, Parkville, Vic
Competing interests: None
Provenance and peer review: Not commissioned, externally peer reviewed
Acknowledgements
The authors would like to thank all volunteer participants for taking part in the study, and to VicReN members for assistance with recruitment of participants. The authors would also like to sincerely thank the Department of General Practice, University of Melbourne, for their tremendous support and assistance in making this study possible.