Long-acting reversible contraceptives (LARC), including intrauterine devices (IUDs) and contraceptive implants, are more effective and cost-effective in preventing unintended pregnancies than most other contraceptive methods.1,2 In spite of this, IUDs are underused in Australia.3,4 Only an estimated 3% of Australian women seeking contraception were using an IUD in 2011.4
Access to IUDs appears to be limited by the lack of community‑based practitioners experienced in inserting these devices. A recent analysis of Australian general practice consultations using data from the Bettering the Evaluation and Care of Health (BEACH) program indicated that 6.9% of all contraception consultations recorded the use of LARC.5 A global review of barriers to widespread use of IUDs among nulliparous women identified that healthcare providers’ attitudes have the most profound effect on uptake.6
IUD inserters in Australia include gynaecologists, general practitioners (GPs), and family planning doctors and nurses. Family planning organisations across Australia offer training in IUD insertion. The skills-based training is a potentially important strategy for increasing the use of IUDs, but such training is intensive, time-consuming and relatively expensive. This study was designed to identify and understand the IUD insertion outcomes of GPs who had undertaken IUD insertion training at Family Planning NSW (FPNSW).
FPNSW has been conducting IUD insertion training programs for GPs for more than 15 years in Sydney, Newcastle and Dubbo, using an approach that is consistent with nationally agreed standards.7,8 The training program is accredited by The Royal Australian College of General Practitioners (RACGP) and Australian College of Rural and Remote Medicine (ACRRM) quality improvement and continuing professional development programs. Competency-based clinical training involves participants inserting IUDs in patients under the supervision of experienced doctors.
Methods
All doctors who enrolled in FPNSW’s IUD insertion training programs in 2012 were invited to participate in the study by completing a pre-workshop questionnaire and a follow-up questionnaire 12 months after completing training. The doctors completed training between April 2012 and February 2013. Follow-up data were collected between June 2013 and April 2014.
The questionnaires examined relevant knowledge, attitudes and barriers to IUD insertion that the doctors anticipated or experienced. The follow-up questionnaire also collected numbers and outcomes of insertions, including adverse events and referrals to external IUD providers. The questionnaire was developed specifically for this study, informed by a review of the literature and piloted internally. The full questionnaire is available in Appendix 1 and Appendix 2 (available online only).
A comprehensive, evidence-based approach to follow-up was implemented.9 This included personalised emails and letters, including paper or electronic options, a gift card to thank participants for their time and follow-up phone calls when necessary.
Data were analysed using SPSS version 19. Normality test was applied for continuous data to examine the distribution. For normally distributed data, differences between means were examined with t-tests; for non-normally distributed data, the Mann–Whitney U test was used to examine the difference between groups. Changes in proportions over time were examined with McNemar’s tests. An effect was considered statistically significant if a two-tailed test resulted in a P value <0.05.
Ethics approval was obtained from FPNSW’s ethics committee (reference 2011-08).
Results
Thirty doctors were enrolled in three IUD insertion training programs, which began in March, July and October 2012. One doctor did not consent to participate in the study and two consented but did not complete the training course. Three other doctors completed the training program, but not within the follow-up time frame. All but one of the enrolled doctors were female, and the sole male participant did not complete training within the follow-up time frame. This left 24 (female) eligible doctors, aged 28–54 years (mean: 42 years of age), to be followed up. Twenty-one doctors worked in private general practice (one also worked in an FPNSW clinic) and one in the Royal Flying Doctor Service remote women’s clinics. One other doctor worked in a hospital and another at a university health service.
None of the doctors were inserting IUDs in their current practice. Seven doctors previously inserted IUDs in Australia or overseas and 16 had never inserted IUDs. Eight were working in practices with other doctors who were IUD inserters.
In the pre-training questionnaire, participants agreed with a variety of listed reasons for undertaking training, including:
- desire for new knowledge and skills – 13 doctors
- patient demand – nine doctors
- difficulty in referring to local IUD providers – five doctors.
Of the 24 doctors who completed the training, 18 (75%) provided both pre-training and follow-up data; 22 (92%) provided follow-up data.
Post-training IUD insertion activity
In the follow-up questionnaire, participants were asked about the number of IUD insertions undertaken in the past 12 months. Nineteen of the 22 participants (86%) who provided follow-up data reported undertaking at least one IUD insertion in that period. Seven participants (32%) reported that they had undertaken 12 or more insertions. In total, the participants undertook 238 IUD insertions (70% hormonal IUDs) during the follow-up period (median = 5.5; interquartile range [IQR] = 15); 212 insertions (89%) were reported to be successful (median = 4.5; IQR = 14; Figure 1).
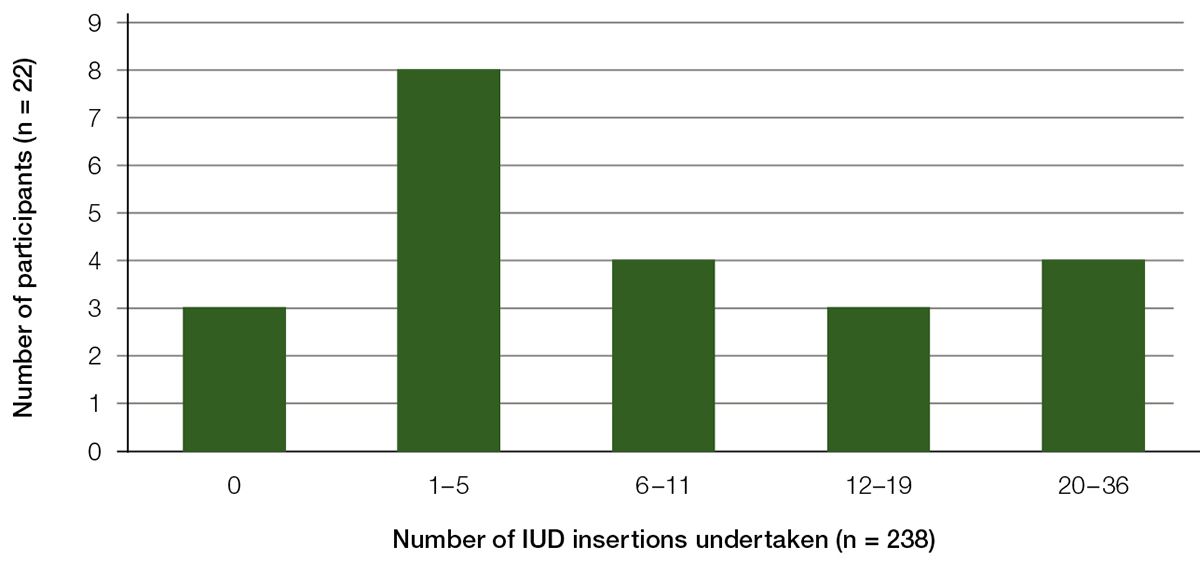
Figure 1. Number of IUD insertions undertaken by participants 12 months post-training
Participants with previous inserting experience undertook a median of 10 insertions (IQR: 14) during the follow-up period, compared with a median of five (IQR = 11) by participants without such experience. This difference was not statistically significant (Z = 0.815; P = 0.415).
Participants who worked in clinics where IUDs were being inserted by other clinicians at the practice at the start of their training (median = 9; IQR = 15) were not significantly more likely to be inserting IUDs at 12 months post-training than those in practices without IUD inserters (median = 5; IQR = 9; Z = 0.823; P = 0.41).
Problems encountered with IUD insertions
Only a few problems related to IUD insertion were reported during the 238 insertions. The most common was uterine sounding problems (10 cases), followed by IUD technical problems (five cases) and vasovagal reactions (four cases). Two IUDs were reported to have been malpositioned and five were reported to have been expelled. There were no reported cases of infection or perforation.
Barriers to inserting IUDs
Participants were asked about barriers to inserting before and after their training (Table 1). There was a statistically significant increase in the perception that IUD insertion was not cost-effective for their practice but no significant difference in the other reported barriers. Of the 22 participants who provided follow-up data, 20 (91%) identified one or more barrier to inserting IUDs, and eleven (50%) identified two or more barriers.
Table 1. Number of doctors who predicted (pre-training) or reported (post-training) having experienced specific barriers
to inserting IUDs
| |
Number of doctors
(paired pre-post samples, n = 18)
|
Significance of difference
(P value, McNemar’s test)
|
|---|
|
Barrier
|
Pre-training (n)
|
Follow-up (n)
| |
|---|
|
Lack of cost-effectiveness for the practice
|
1
|
8
|
0.016
|
|
Time constraints
|
3
|
7
|
0.130
|
|
Lack of suitable patients
|
1
|
6
|
0.063
|
|
Level of confidence inserting unsupervised
|
3
|
5
|
0.730
|
|
Lack of equipment
|
7
|
3
|
0.290
|
|
Need for nurse assistance
|
3
|
3
|
1.000
|
Table 2. Confidence in inserting IUDs at the 12 months follow-up
|
Clinical scenario
|
Number of ‘Strongly agree’/‘Agree’ (%)
|
95% confidence interval
|
|---|
|
I have confidence and skills to insert hormone bearing IUDs (Mirena) in multiparous women
|
21/22 (96%)
|
0.772–0.999
|
|
I have confidence and skills to insert copper IUDs in multiparous women
|
14/22 (64%)
|
0.407–0.828
|
|
I have confidence and skills to insert hormone bearing IUDs (Mirena) in nulliparous women
|
10/22 (46%)
|
0.244–0.678
|
|
I have confidence and skills to insert copper IUDs in nulliparous women
|
5/21 (24%)
|
0.082–0.472
|
In the follow-up questionnaire, the participants completed five-point Likert scales to rank their confidence and skill in inserting IUDs. Confidence was greater for hormonal IUDs and for multiparous women. Nearly all participants (96%) were confident in inserting hormonal IUDs in multiparous women; 64% indicated confidence for copper IUDs in multiparous women; and 46% for hormonal IUDs in nulliparous women. Only one-quarter (24%) indicated confidence in inserting copper IUDs in nulliparous women (Table 2).
In the follow-up questionnaire, participants were asked to estimate the number of patients they referred to other practitioners to have IUDs inserted in the three months before starting IUD insertion training (multiplied by four to give a 12-month estimate), and in the 12 months post-training. Eighteen participants (82%) estimated that they made fewer referrals in the 12 months post-training (median = 2.5; IQR = 16) than in the three months pre-training (median = 20; IQR = 28). The difference was statistically significant (Z = 3.251; P = 0.0011).
Discussion
With a 92% follow-up rate, this study is one of few that have provided data regarding outcomes of IUD insertion training. Our training program was successful in supporting GPs who were not currently inserting IUDs in their practice to implement this skills-based practice in their setting. It has been suggested that doctors who insert IUDs need to insert at least 12 per year to maintain their skills.10,11 The 22 doctors in this study undertook 238 IUD insertions in the 12-month follow-up period. However, only seven (32%) achieved 12 or more insertions in that time frame. The number of insertions undertaken was not significantly associated with previous inserting experience or working with other IUD-inserting doctors. Insertion attempts in this study were successful in 212 cases (89%), which is slightly lower than rates reported among experienced inserters. A comparison with our findings is provided by a study of 996 IUD insertion attempts by experienced doctors at Family Planning Queensland and FPNSW clinics, of which 95.5% were successful.12 Six other studies reported success rates by various healthcare practitioners ranging from 95.2 to 99.5%.13–18
Our study participants reported a low incidence of complications associated with their insertions. However, many of our participants indicated lack of confidence regarding IUD insertions in nulliparous women. There is mixed evidence for the difficulty of inserting IUDs in nulliparous women. Three previous studies recorded successful insertion rates of 6–9% higher among parous women than nulliparous women.12,17,19 However, two other studies of IUD insertions in nulliparous women recorded success rates of 95%18 and 96%,15 and another study reported a 99% insertion success rate with young university students.13 Three further studies found only small differences between parous and nulliparous women in terms of clinicians’ ratings of insertion difficulty.12,14,16 It may be that increased practise improves confidence. Additionally, a lack of confidence in inserting copper IUDs is likely to reflect the higher usage of hormonal IUD among women, and the fact that the techniques for each are different.
In order to build and maintain confidence in IUD insertion, including insertion in nulliparous women and the use of copper IUDs, there may be a role for an expansion of designated IUD clinics at family planning clinics and clinics attached to public hospital outpatient departments. This could increase IUD insertion opportunities for trained primary care doctors as well as access for women. This model would also facilitate the creation of a community of practice of IUD inserters.
Nearly all participants reported encountering barriers to incorporating IUD insertion into their practice. These included cost barriers in their practices, time constraints and low patient numbers. Remuneration needs to be satisfactory for the time taken for training, preparation and the consultation itself. The Medicare Benefits Schedule (MBS) fee for IUD insertion is $53.55. The fee for IUD insertion is relatively low considering the training and skill involved, the equipment required and the potential cost of having an assistant (eg practice nurse or assistant in nursing). In the UK, financial incentive schemes have been introduced to general practice that have increased the uptake of LARC methods.20 The cost-effectiveness of training nurses to insert IUDs could also be explored.21
The lack of suitable patients reported by some participants needs to be further explored. In the FPNSW clinical setting, there is a high demand for IUD insertion appointments. Implementing referral pathways within primary care networks to GPs who are trained in IUD insertion could potentially increase access for women and support maintenance of skills.
Translation of training into practice may have been challenging for some of the participants. Alternative models where training is provided in the GP’s own practice may have a role.22 This may overcome confidence and implementation barriers.
Following their insertion training, participants reported that they referred significantly fewer patients to other practitioners to have IUDs inserted. There may be many factors at play such as recall bias and improved awareness of IUD suitability.
Limitations of the study
Although the response rate in the study was high, it only involved a small number of doctors, which limited analysis of some issues. Failure to detect a statistical difference may be due to a lack of statistical power. The data reported in this paper are based on recall and estimates rather than prospective collection or clinical file audit, and may have been affected by recall and social desirability bias. Other IUD insertion outcome studies that were based on file audit or did not specify their follow-up contact rate have had similar limitations of possible under-reporting and missing data.14,17,19 Given that most of the study participants undertook small numbers of IUD insertions, we consider that recall would have been adequately accurate.
Implications for general practice
The training of primary care practitioners is an essential step in ensuring that women requesting IUDs can have them inserted in a timely manner. GPs who undertook FPNSW’s IUD insertion training program report high levels of confidence; however, there remain significant barriers to the delivery of such services after training. The main barriers are concerns about remuneration, time constraints and patient demand for services. The reported lack of confidence in inserting IUD in nulliparous women may reflect practitioners’ concerns regarding potential difficulty or adverse events, as well as low community awareness. Increased awareness of the suitability of IUDs for nulliparous women is needed.
The issue of skill maintenance may be overcome by implementing referral pathways within primary care networks for GPs to refer patients to their colleagues.
Consideration can be given to other models of training and delivery of service to develop and maintain a primary care workforce that is competent and confident in providing IUD insertion. This is an important step in increasing access to and uptake of this method of reversible contraception that has the potential to decrease rates of unintended pregnancies.
Authors
Mary Stewart MBBS, DFSRH, MPH (Public Health), Senior Medical Officer: Research and Education, Family Planning, Ashfield, NSW. marys@fpnsw.org.au
Erol Digiusto BSc (Hons), PhD, Senior Research Officer, Family Planning, Ashfield, NSW
Deborah Bateson MA, MSc, MBBS, Medical Director, Family Planning, Ashfield, NSW; Clinical Associate Professor, Discipline of Obstetrics, Gynaecology and Neonatology, University of Sydney, Camperdown, NSW
Rebecca South MBBS, FRACGP, DRANZOG, IUD Training Coordinator, Family Planning, Ashfield, NSW; General Practitioner, The Leichhardt General Practice, Leichhardt, NSW
Kirsten I Black MBBS, MMed, FRANZCOG, DDU, PhD, MFSRH, Associate Professor, Discipline of Obstetrics, Gynaecology and Neonatology, University of Sydney, Camperdown, NSW; Women’s and Babies, Royal Prince Alfred Hospital, Camperdown, NSW
Competing interests: This study received no external funding; however, Bayer Healthcare provided the initial funding for the FPNSW IUD insertion training course in 2009. Bayer Healthcare additionally provided sponsorship for 17 of the participating doctors to cover the cost of their training. FPNSW also receives sponsorship for its educational courses from Bayer Healthcare. Deborah Bateson has been supported to attend conferences and expert advisory panels by Bayer Healthcare, but has never received personal remuneration for these services.
Provenance and peer review: Not commissioned, externally peer reviewed.
Acknowledgements
We would like to acknowledge the doctors who participated in the training and agreed to take part in this research. We would also like to acknowledge the Family Planning NSW librarian, Amanda Young, for her assistance with referencing.