Hoarseness, a general term used to describe any change in the character of a patient’s voice, is a common presenting complaint among all population groups. It is estimated to affect up to one-third of the adult population1 at some point in their lives and one-tenth of children.2 Diagnosing and treating the cause of hoarseness can be difficult. This article will outline an approach to assessing hoarseness, discuss management of common benign causes and when to refer to an otorhinolaryngologist.
Anatomy and physiology
Voice requires four components:
- the lungs to provide a sufficient air stream through the vocal cords
- the larynx and, specifically, the vocal cords to create the sound
- the resonance chamber made up of the pharynx, nasal and oral cavities, which project the sound
- the nervous system, which provides overall control.
Pathology of any one of these components may affect a person’s voice.
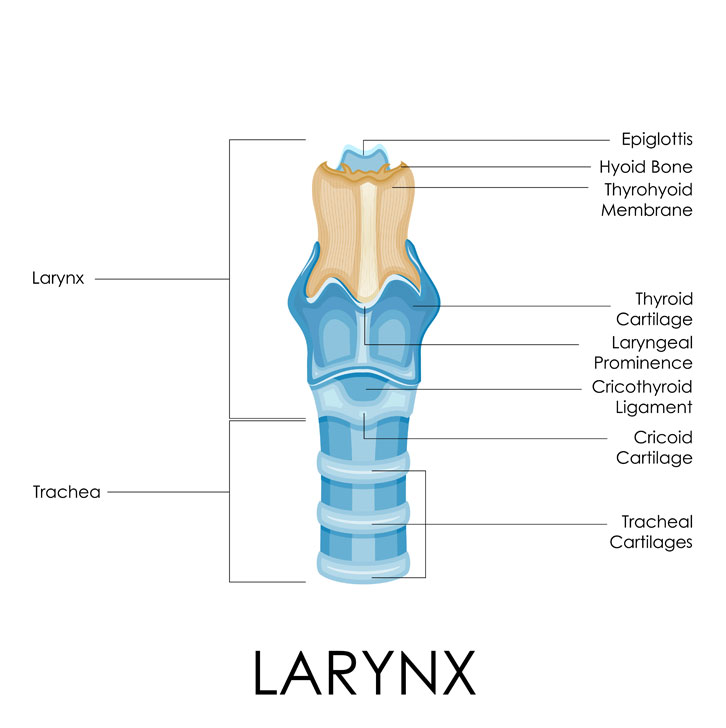
The larynx is a complex structure that stretches from the base of the tongue to the trachea and lies opposite the third to sixth cervical vertebrae (Figure 1).3 It consists of three single cartilages: the thyroid, cricoid and epiglottic; and three paired cartilages: the arytenoid, cuneiform and corniculate cartilages, interconnected by ligaments and muscles. There are synovial joints between the thyroid and cricoid cartilages and the cricoid and arytenoid cartilages. These can occasionally be affected by joint disease, such as rheumatoid arthritis or systemic lupus erythematosus.
 |
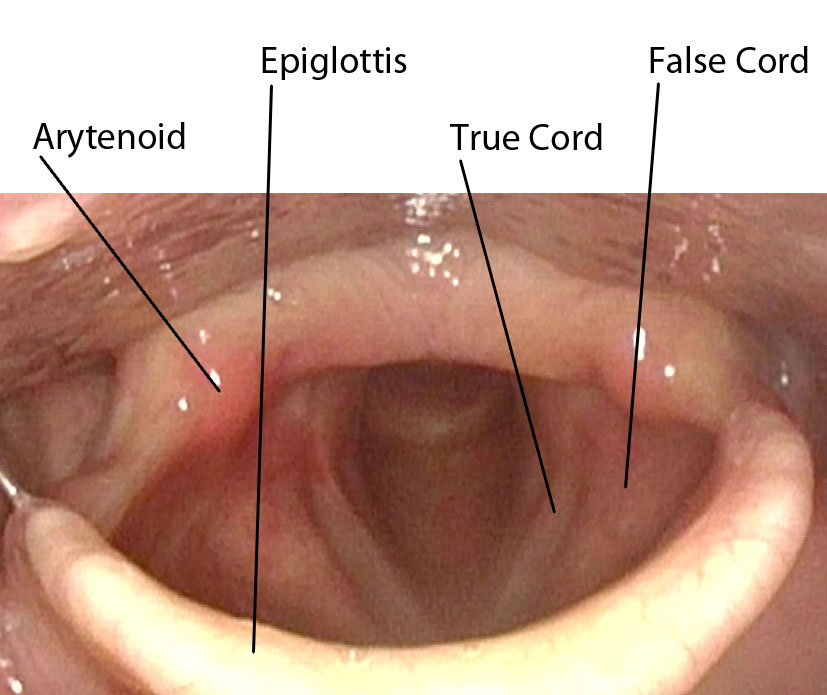 |
Figure 1. Anatomy of the larynx
Reproduced with permission from Shutterstock Netherlands |
Figure 2. Internal view of the larynx during inspiration |
Deep within the larynx are the vocal cords, which create the sound (Figure 2). The vocal cords are made up of multiple layers and voice is created by vibrations of the outer layers due to the passing air. Damage to any of these layers or the space between the layers can affect the voice. An example of this is Reinke’s oedema, an oedema of the superficial lamina propria that results in a deep voice and is most commonly caused by smoking and voice overuse.
All of the intrinsic muscles of the larynx (except cricothyroid) are innervated by the recurrent laryngeal nerve (RLN). The course of the RLN is complex and leaves it vulnerable to damage during cervical and thoracic procedures. After leaving the vagus nerve, on the right it loops around the subclavian artery and on the left around the aortic arch, then ascends slightly anterior to the tracheoesophageal groove to where it enters the larynx. The left RLN is more commonly injured, most likely because of the longer course. Damage of the nerve may be due to apical lung masses, direct injury during trauma or surgery, post-operative oedema and, occasionally, unknown aetiology.
History
Taking a history from a patient presenting with hoarseness is similar to any other presenting complaint. Important red flags include a history of smoking, dysphagia, odynophagia or otalgia, stridor, haemoptysis and recent fevers, night sweats and unexplained weight loss.4,5 If any of these are present and the hoarseness is persistent, an urgent referral to an otorhinolaryngologist should be made. Hoarseness that is intermittent in nature is less likely to be due to a fixed lesion.6
History should include the presence of heartburn or any recent upper respiratory tract infections. If a patient is using a steroid inhaler, check how they use it and if gargling is performed after each use. Ascertain if the patient has had any recent surgery or trauma to the neck or chest as the RLN may have been damaged. Similarly, a recent intubation (especially if prolonged or traumatic) may have resulted in laryngeal injury. Associated systemic diseases can include hypothyroidism, neurological disease such as Parkinson’s disease or myasthenia gravis, and inflammatory or autoimmune conditions, such as rheumatoid arthritis. Professional voice users are particularly prone to voice hoarseness. Social history should include both work as well as co-curricular activities.
Examination
The examination for hoarseness can be difficult because the larynx cannot be visualised. Many differential diagnoses can be excluded with a thorough head, neck and chest examination. First, listen to the voice and note the quality, pitch and volume. Table 1 provides some examples of common voice changes and associated diagnoses.7,8 During this period, ask the patient to sustain the vowel sound ‘ah’ for as long as they can and time it. This maximal phonation time can vary, but if less than eight seconds it often indicates an organic pathology.9 Ask the patient to cough and listen to the quality. If the cough is breathy and ineffective it can suggest poor glottic closure and an impairment of vocal cord movement.
Table 1. Possible causes based on description
|
| Voice quality | Possible cause |
|---|
| Deep |
- Reinke’s oedema
- Hypothyroidism
|
| Raspy |
|
| Intermittent |
|
| Gravelly |
- Vocal cord mass
- Inflammatory arthritis
|
| Soft |
- Parkinson’s disease
- Vocal cord paralysis
|
| Fatiguable |
- Muscle tension dysphonia
- Myaesthenia gravis
- Parkinson’s disease
- Phonotrauma
|
| Strained or strangled |
- Spasmodic or muscle tension dysphonia
|
During the respiratory examination, listen for stridor. This is a worrying sign of airway obstruction and should prompt urgent referral for direct visualisation. Decreased lung expansion and auscultation may indicate a restrictive lung pathology that is affecting the volume of air passing through the larynx and hence a patient’s voice.
Oral cavity and oropharyngeal examination may identify lesions that affect the resonance chamber and hence a patient’s perception of a voice change. In particular, examine and palpate the base of the tongue and tonsils. A cranial nerve examination should also be included as it may indicate a central pathology. Further neurological examination should be considered if the history is suggestive of a central or neurological pathology. Palpate the neck and thyroid for any masses. Additional system examinations would be indicated if any systemic causes are suspected. If the practitioner is experienced in the procedure, indirect laryngoscopy may be useful.
Investigation and management
There are no clinical practice guidelines in Australia, but the United Kingdom National Institute for Health and Care Excellence (NICE) guidelines10 suggest that any patient over 45 years of age with unexplained, persistent hoarseness should be referred to a specialist for further investigation. The urgency of the referral should reflect concurrent symptoms and associated red flags, but it is recommended that any persistent hoarseness, present for more than three weeks, requires referral for direct visualisation.5,6
Figure 3 outlines a basic algorithm for referral and management of common benign pathologies. Any suspicious mass should be investigated with imaging and a fine needle aspiration and referred to an otorhinolaryngologist for ongoing work-up and management. Imaging is not recommended prior to visualisation of the larynx if the remaining examination has been unremarkable.11
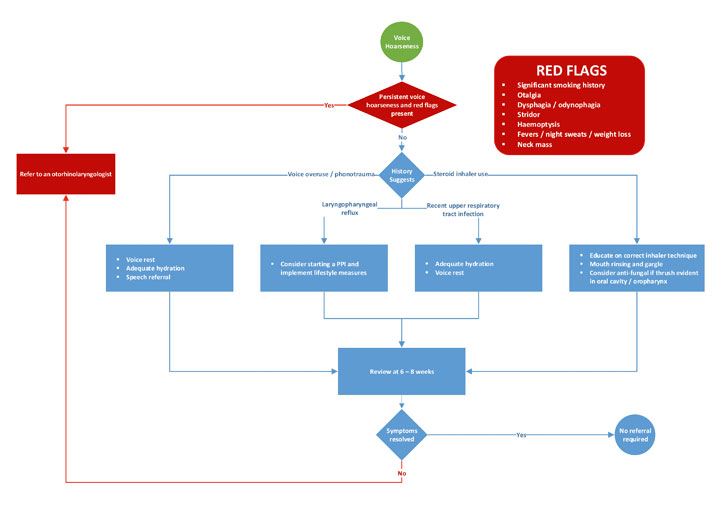 |
Figure 3. A hoarseness algorithm
PPI, proton pump inhibitor |
If the history and examination suggest voice overuse or phonotrauma, voice rest should be recommended.9 It is important to educate patients that whispering is no better for the voice and should also be avoided. A referral for speech therapy will be particularly important for those patients who use their voice professionally.8 Vocal fold hydration by high fluid intake and steam inhalation or humidifiers has been shown to be an important component in improving the condition and efficiency of the vocal cords.7,8 Other vocal hygiene strategies include smoking and alcohol cessation and reducing caffeine intake.
A patient with laryngopharyngeal reflux (LPR) usually presents with a raspy voice. The most common additional symptoms are heartburn and chronic throat clearing.12 A trial of proton pump inhibitors and implementing lifestyle measures to limit the reflux should be initiated.5 Recent studies have shown that laryngopharyngeal reflux is overdiagnosed13 and if symptoms do not resolve after a trial of the management strategies mentioned above, a referral to an otorhinolaryngologist should be made and an alternative diagnosis pursued. LPR may also co-exist with more malignant pathology.
Laryngitis usually follows symptoms of an upper respiratory tract infection or short-term vocal abuse.8 There may be a history of previous episodes. A simple viral laryngitis is usually self-limiting and should resolve within three weeks.5 During this time encourage voice rest, adequate hydration and vocal hygiene. Sucking lozenges may also help.
Steroid inhaler laryngitis is common and often easily treatable. Ensure the patient is using the inhaler in the correct manner and not only rinsing their mouth but also gargling after each use. If oral thrush is evident on examination of the oral cavity and oropharynx it would be reasonable to start an antifungal medication. The patient may also complain of sensitivity to hot and spicy food. Reassess the need for the steroid inhaler and, if needed, the dose, as cessation or reduction of inhaler use has been shown to be the most effective treatment.14
Conclusion
Hoarseness is a common presenting complaint and can be a symptom of benign or malignant disease. It is important to differentiate between those requiring urgent referral to an otorhinolaryngologist and those who can be safely managed by the general practitioner. Vocal hygiene and speech therapy are valuable treatment tools for many benign conditions. Any patient with red flag features on history or persistent hoarseness should be referred to an otorhinolaryngologist.
Authors
Lauren N Cooper BPhty, MBBS, Ear, Nose and Throat Principal House Officer, Ear, Nose and Throat Department, Ipswich Hospital, Ipswich, QLD. lncooper@icloud.com
Rachele A Quested BPhty, MPHty, MBBS, Junior House Officer, Ear Nose and Throat Department, Ipswich Hospital, Ipswich QLD; University of Queensland School of Medicine, QLD
Competing interests: None.
Provenance and peer review: Not commissioned, externally peer reviewed.