Case
A man, aged 32 years, presented to his general practitioner (GP) with a one-month history of increasing bilateral breast swelling (Figure 1). He was distressed by the appearance and said there was some pain on breast palpation. He denied any other symptoms and was usually healthy.
 |
| Figure 1. Patient’s breast swelling |
Question 1
What are the causes of breast swelling in males?
Question 2
How would you differentiate the possible causes?
Answer 1
There are many possible causes of male breast swelling. A common cause is gynaecomastia, which is the benign proliferation of glandular breast tissue in males. It is frequently encountered by primary care physicians as a result of the patient’s cosmetic concerns or pain.1 Breast malignancy is the most concerning diagnosis of breast swelling. Other causes include pseudogynaecomastia (fat without glandular proliferation), lipoma, sebaceous cyst, dermoid cyst, fat necrosis and haematoma.2
Answer 2
In true gynaecomastia, a rubbery or firm tissue that is concentric with the nipple–areolar complex is palpable. It is usually bilateral, although it can be unilateral. Features of breast malignancy classically include a stony hard, immobile, non-tender, unilateral mass with potential skin dimpling, nipple retraction, nipple discharge and axillary lymphadenopathy.2 Bilateral male breast cancer is rare (approximately 1.5% of all male breast cancer), and synchronous bilateral male breast cancer is extremely rare (<0.5% of all male breast cancer).3 In some cases, it may be challenging to distinguish between gynaecomastia and breast malignancy purely on palpation. If there is any uncertainty, triple assessment with mammography and biopsy is required.2
Case continued
You note that this patient has features of true gynaecomastia.
Question 3
What are the common underlying causes of gynaecomastia? What would you want to elicit from history and examination in a patient with gynaecomastia?
Answer 3
Gynaecomastia occurs as a result of an imbalance in the free oestrogen to free testosterone ratio that is secondary to a variety of physiological and non-physiological causes. The common age groups for physiological gynaecomastia are newborn babies (0–3 weeks; 60–90%), adolescents (10–17 years; 50–60%) and older men aged 50–69 years (35–65%). Be particularly wary of non-physiological gynaecomastia when patients are outside of these age groups have gynaecomastia that is recent in onset, progressive or of unknown duration.4–6
The most frequent non-physiological cause is medications, although there are numerous differentials to consider (Table 1).7,8 Keeping these aetiologies of gynaecomastia in mind, take a thorough medication history, and assess for signs of:1,2
- cirrhosis (jaundice, ascites, pruritus)
- malnutrition
- chronic renal failure (oedema, fatigue)
- hyperthyroidism (weight loss, palpitations, fine tremor)
- hypogonadism (erectile dysfunction, decreased muscle mass, testicular atrophy)
- testicular tumours (testicular mass)
- adrenal tumours (abdominal mass).
|
Table 1. Causes of gynaecomastia
|
|
Medications
- Cardiovascular
- Spironolactone
- Digoxin
- Amiodarone
- Hormonal
- Anti-androgens (eg bicalutamide, flutamide)
- Oestrogens
- Gonadotropin-releasing hormone (GnRH) agonists
- 5-alpha reductase inhibitors (eg finasteride, dutasteride)
- Antimicrobials
- Ketoconazole
- Metronidazole
- Psychoactive
- Haloperidol
- Diazepam
- Tricyclic antidepressants
- Chemotherapy
- Alkylating agents
- Methotrexate
- Recreational
- Alcohol
- Tetrahydrocannabinol (THC; marijuana)
- Anabolic steroids
Idiopathic
Cirrhosis
Malnutrition
Hypogonadism (primary or secondary)
Tumours secreting hCG or oestrogen/oestrogen precursors (eg testicular or adrenal tumours)
Chronic renal failure
Hyperthyroidism
|
Case continued
You find a right-sided testicular lump. It is asymmetrical, firm, hard and non-tender. The patient denies noticing this lump previously. There were no other significant findings on history or examination.
Question 4
What investigations would you order?
Answer 4
A testicular neoplasm may be responsible for the patient’s gynaecomastia. Approximately 10% of testicular tumours present with gynaecomastia as the only symptom, and about 2% of men with gynaecomastia are found to have testicular neoplasms.9 While there is probably a low likelihood of a positive result, some guidelines recommend that all patients with true gynaecomastia (aside from newborn babies) undergo liver function tests (for evidence of cirrhosis), thyroid function tests (for hyperthyroidism) and electrolytes/urea/creatinine (for chronic renal failure).1 Other sources state that patients deemed to have physiological gynaecomastia after careful history and examination do not require further investigations, and can simply be re-evaluated in six months.8
As a non-physiological cause of gynaecomastia is likely in this case, and medications are not involved, blood tests should be performed to check levels of the following (ideally with a morning sample given the pulsatile nature of these secretions):2
- blood human chorionic gonadotropin (hCG)
- luteinising hormone
- follicle stimulating hormone
- testosterone
- oestradiol
- prolactin.
Testicular cancer serum markers (alpha-feta protein and lactate dehydrogenase) must also be tested in this case. Furthermore, a scrotal ultrasound is mandatory to further characterise the testicular lump.2
Case continued
The biochemistry reveals significantly elevated human chorionic gonadotropin (hCG), oestradiol and testosterone. The scrotal ultrasound is consistent with a right-sided testicular malignancy (Figure 2).
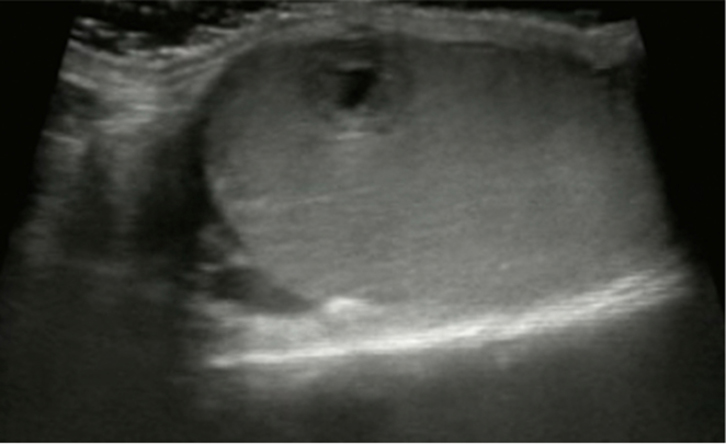 |
| Figure 2. Scrotal ultrasound showing a heterogeneous mass in the right testicle with a mixed cystic/solid appearance |
Question 5
How does testicular cancer cause gynaecomastia?
Question 6
How would you manage this patient?
Answer 5
Testicular malignancies are classified as either germ cell (95%) or sex cord stromal (5%) in origin – each causes gynaecomastia via different mechanisms.10 Germ-cell tumours that have a choriocarcinoma component secrete hCG, resulting in Leydig cell dysfunction and, in turn, increases in both oestradiol and testosterone production. The rise in oestradiol is relatively greater than testosterone.11
Leydig cell tumours (a type of sex cord stromal tumour) are rare, but are more likely to cause gynaecomastia because they directly secrete more oestradiol and convert additional androgen precursors to oestrogens.10,11
Answer 6
The patient has clinical, biochemical and ultrasound features consistent with testicular cancer. He requires a chest X-ray (for evidence of widespread lung metastases) and urological review within two weeks. The urologist will arrange sperm banking and radical inguinal orchiectomy for histological diagnosis. The patient will also need to undergo appropriate staging investigations including computed tomography (CT) scans of the chest, abdomen and pelvis scans for evidence of lymph node and distant metastatic spread. If there is clinical suspicion of cerebral or bone metastases, he will need to undergo brain magnetic resonance imaging (MRI) and/or bone scan. Subsequently, the patient’s case will be discussed at a multidisciplinary team meeting to determine further treatment (if required).12
Key points
- Male breast swelling is a relatively common general practice presentation with a broad differential. Two important causes to consider are gynaecomastia and breast malignancy.
- Gynaecomastia can be purely physiological, but may be a sign of sinister underlying pathology such as testicular cancer.
- A systematic evaluation, including history, examination and pertinent investigations, can effectively identify such pathology.
Authors
Nandu Dantanarayana MBBS (Hons), MS, Surgery, St Vincent’s Hospital, Darlinghurst, NSW. nandu.dantan@gmail.com
Joanna Connolly MBBS (Hons), Medicine, Royal Prince Alfred Hospital, Camperdown, NSW
Competing interests: None.
Provenance and peer review: Not commissioned, externally peer reviewed.