Patterns of abuse
Prescription drug abuse is a worldwide problem of increasing concern to governments and the United Nations.1 Research data indicate that prescription drug abuse is increasing in Australia. The 2013 National Drug Strategy Household Survey (NDSHS) found that 4.8% of Australian adults used pharmaceuticals for non-medical purposes in the past 12 months, an increase from 3.8% in 2004.2 The number of people in needle and syringe programs who reported that the drug they last injected was a prescription opioid increased from 7% in 2000 to 23% in 2015.3 The two most common types of drugs abused were analgesics and sedatives. These two drug types can activate the reward regions in the brain by increasing dopamine neurotransmitter levels, which in turn can generate a feeling of pleasure and relief of dysphoria.
The type of drugs being abused changes over time, often depending on availability. Legislative changes by governments and marketing decisions by pharmaceutical companies are two important factors that can alter availability and perceptions about particular drugs. For example, the Australia-wide rescheduling of alprazolam from a schedule 4 to schedule 8 drug in 2014 led to a 35% reduction in the number of scripts dispensed in the first 12 months.4 By contrast, changes in attitudes to opioid use towards the end of the 20th century and the subsequent increase in use have been well documented in many Western countries.5 Australian opioid dispensing episodes increased from 500,000 prescriptions in 1992 to 7.5 million prescriptions in 2012.4,6
In 2015, a survey conducted by the National Drug and Alcohol Research Centre (NDARC) of Australian residents who regularly injected illicit drugs found that the most common prescription drugs they injected were slow-release morphine capsules and benzodiazepines. A small number of participants reported that they had injected other prescription drugs, such as fentanyl, codeine, pharmaceutical stimulants or quetiapine, in the previous six months.7
Prescription drug misuse and abuse can take varying forms, and different definitions have been used to try to categorise these behaviours. Drug misuse can be defined as use contrary to the prescribed instructions, without regard to any resulting harm or adverse effects. Drug abuse can be defined as intentional use of the drug for a non-medical purpose, such as euphoria or to alter one’s state of consciousness.5
Drug-related deaths
One way of assessing drug abuse and its related harms is to look at the worst possible outcome – death. The coroner investigates all unexpected deaths in Victoria (population 5.9 million). Each year, about 6000 cases are investigated and all bodies are screened for a wide range of drugs. The Coroners Court of Victoria defines an overdose death as ‘any death in which the acute toxic effects of one or more drugs played a causal or contributory role’.8 On the basis of all the available data for that death, the forensic pathologist or toxicologist decides whether the drug is causal or contributory.
Summary data released by the Coroners Court of Victoria on overdose deaths concluded that the number has risen from 379 in 2009 to 453 in 2015.8 This is more than double the fatal road toll in Victoria for 2015. Importantly, most overdose deaths are actually due to combined drug toxicity – the fatal mixture of two or more drugs used together. Comparing annual overdose deaths in Victoria from pharmaceuticals to those from illicit drugs and alcohol demonstrates that between 2009 and 2015, pharmaceuticals consistently played a role in around 80% of deaths each year. Illegal drugs contributed to around 40% of the annual overdose deaths. Alcohol contributed to an average of 25% deaths (Table 1).8
The coroner’s data also show that benzodiazepines were the most frequent contributing drug group, contributing to an annual average of 51.3% of all overdose deaths during 2009–15. Opioid analgesics contributed to an annual average of 48.5% during that time (Table 2).
Table 1. Annual overdose deaths frequency by contributing drug types, Victoria 2009–158
|
Drug types
|
2009
|
2010
|
2011
|
2012
|
2013
|
2014
|
2015
|
|---|
|
All overdose deaths
|
379
|
342
|
362
|
367
|
380
|
387
|
453
|
|
Pharmaceutical
|
295
|
266
|
275
|
306
|
313
|
316
|
358
|
|
Illegal
|
147
|
149
|
153
|
133
|
166
|
164
|
227
|
|
Alcohol
|
94
|
85
|
88
|
80
|
94
|
94
|
106
|
|
Reproduced from Coroners Court of Victoria. Findings Case 408012, Attachment C. Coroners Prevention Unit, Coroners Prevention Unit Data Summary, Re: Victorian Overdose Death 2009–2015. Last revised 30th August 2016. Available at www.coronerscourt.vic.gov.au/home/coroners+written+findings [Accessed 6 November 2016].
|
Table 2. Overdose deaths by individual contributing drugs 2009–15, opioids and benzodiazepines8
|
Drug types
|
2009
|
2010
|
2011
|
2012
|
2013
|
2014
|
2015
|
|---|
|
All overdose deaths
|
379
|
342
|
362
|
367
|
380
|
387
|
453
|
|
Contributing drug: benzodiazepines
|
160
|
169
|
180
|
199
|
212
|
215
|
238
|
|
Diazepam
|
104
|
109
|
124
|
133
|
164
|
169
|
192
|
|
Oxazepam
|
18
|
19
|
44
|
41
|
17
|
19
|
34
|
|
Alprazolam
|
62
|
56
|
43
|
57
|
45
|
28
|
23
|
|
Clonazepam
|
7
|
9
|
14
|
18
|
19
|
25
|
33
|
|
Contributing drug: opioids
|
177
|
145
|
183
|
212
|
192
|
186
|
199
|
|
Oxycodone
|
41
|
39
|
46
|
46
|
61
|
46
|
58
|
|
Codeine
|
76
|
57
|
66
|
93
|
71
|
54
|
64
|
|
Morphine
|
22
|
11
|
10
|
13
|
7
|
12
|
8
|
|
Methadone
|
50
|
55
|
72
|
75
|
70
|
67
|
67
|
|
Buprenorphine
|
3
|
4
|
14
|
4
|
3
|
7
|
4
|
|
Reproduced from Coroners Court of Victoria. Findings Case 408012, Attachment C. Coroners Prevention Unit, Coroners Prevention Unit Data Summary, Re: Victorian Overdose Death 2009–2015. Last revised 30th August 2016. Available at www.coronerscourt.vic.gov.au/home/coroners+written+findings [Accessed 6 November 2016].
|
Benzodiazepines
Australia has a publically funded universal healthcare scheme known as Medicare, under which the Pharmaceutical Benefits Scheme (PBS) provides subsidised prescription drugs. Around 80% of all prescription drugs dispensed in Australia are subsidised by the PBS.9 Close to seven million prescriptions for benzodiazepines are dispensed in Australia each year under this scheme, and their main indications for use are short-term treatment of anxiety and insomnia.10 However, such high rates of ongoing benzodiazepine prescribing indicate it is used for long-term problems.11 This is of concern given evidence of its association with addiction, overdose and other harms such as falls (particularly in the elderly) and motor vehicle accidents.12
Benzodiazepines were reported to be the second most commonly misused class of medications, after analgesics, in the 2013 NDSHS.2 Diazepam, the most commonly prescribed benzodiazepine, is also the most common benzodiazepine found at post-mortem (Table 2). The reason why benzodiazepines appear relatively safe on their own but have such a fatal outcome when combined with opioids is still not well understood. It is now recognised that benzodiazepines and opioids interact with the CYP3A4 enzyme system. Scientists have speculated that in the presence of benzodiazepines, the metabolism of opioids is diminished, leading to higher concentrations of opioids and their metabolites, which depress the respiratory system. However, recent studies show little effect on methadone metabolism from benzodiazepines and suggest that pharmacodynamic interactions involving multiple intoxicating drugs, as well as clinical factors, may be more likely to contribute to the death.13
In Australia, general practitioners (GPs) are the main sources of benzodiazepines for 61% of those patients who misuse them.14 It is opportune that in view of the problems associated with this class of drugs that The Royal Australian College of General Practitioners (RACGP) released new guidelines in 2015 on prescribing benzodiazepines in general practice. The guidelines give information on safe prescribing and non-drug alternatives to benzodiazepines.15
Opioids
Prescribing data from the PBS have shown that the total number of dispensed scripts for opioids, particularly the slow-release oral formulation oxycodone, has continued to rise during the 2010–15 period (Figure 1).9 Reasons for the increased volume of opioid prescribing are now a much discussed topic in the lay and medical literature. Multiple factors have been identified as possible causes for this phenomenon, including:
- longer cancer survival periods
- growing group of elderly people with chronic pain from arthritis
- changing community expectations of living with chronic pain
- undertreated mental health issues
- aggressive promotion of potent analgesic drugs by pharmaceutical companies.16
GPs are often left with trying to find the right balance for their patients between pharmaceutical interventions, physical therapies and lifestyle changes.17,18
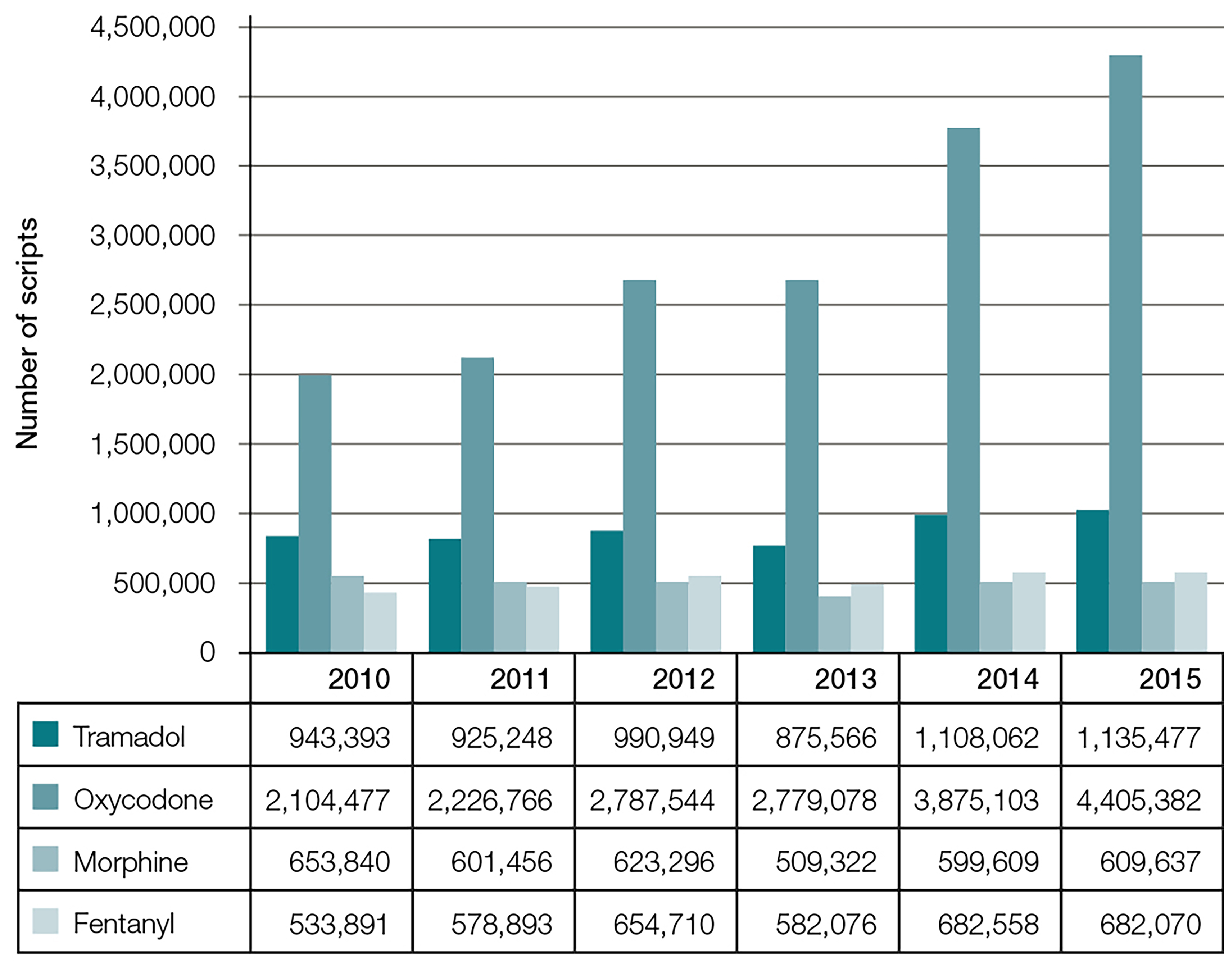
Figure 1. PBS script numbers of certain opioids in Australia, 2010–159 9
Other opioids: Codeine
Since 2009, the Coroners Court of Victoria has reported more than 50 deaths per year where codeine was a contributing factor (Table 2). This highlights the problem associated with abuse of this short-acting opioid analgesic.
In 2013, more than 27 million packs of codeine were sold; 55.8% of these were over the counter and the rest were prescribed.19 Most of this codeine is combined with ibuprofen, paracetamol or aspirin, which in high doses can cause multiple medical and surgical problems. Growing numbers of patients with codeine dependence are attending general practices, hospitals, and drug and alcohol clinics seeking treatment.20
Studies in Australia and overseas have shown that those who misuse codeine often differ in a number of significant ways from users of illicit drugs. They tend to be better educated, more often employed and do not use illicit drugs. They initially use codeine as an analgesic, but then find it helpful as an anxiolytic and mild euphoriant, and eventually become physically and psychologically dependent on it.21 Treatment for codeine dependence has been poorly researched so far, but a recent study in New South Wales has found that a sublingual buprenorphine maintenance program is a useful treatment option for those who cannot stop using codeine compounds.22
Methadone and buprenorphine
Methadone and buprenorphine treatment programs have been a very important part of Australia’s drug and alcohol strategy since the 1970s. More than 48,000 people in Australia were on a program in 2015 (21 clients per 10,000 population). This penetration of the illicit drug use scene has been credited, together with the needle exchange program, of saving the country from a human immunodeficiency virus (HIV) epidemic among injecting drug users. The harm reduction approach of the treatment programs has continued to save lives and reduce crime.23,24
In Victoria, there were 14,122 people on opioid pharmacotherapy programs in mid-2015, with 4819 (34%) on buprenorphine (either buprenorphine tablets or buprenorphine/naloxone wafers) and the rest on methadone.24 Abuse of methadone syrup and buprenorphine tablets and wafers does occur, as medications can be injected, diverted to friends or sold on the black market.25 Suboxone tablets can be crushed and injected, and methadone syrup can also be injected (especially if undiluted). In particular, diversion (giving or selling to another person) of take-home doses of methadone has come to the attention of the coroner as deaths from this practice have risen.3
Methadone-related deaths cause heightened community and medical concerns because of ongoing debates about opioid replacement therapy, the risk of medication diversion, and the doctor’s role in prescribing and monitoring patients. In the triennium 2013–15, a total of 204 methadone-related deaths were detected by the Coroners Court of Victoria, compared with 14 buprenorphine-related deaths in that same period.26 Table 3 shows the risk calculation for overdose deaths on the program.
Table 3. Overdose death rates on methadone and buprenorphine program in Victoria, 2013–20158,35
|
Drug
|
Total number of deaths 2013–15
|
Number on program (average)
|
Deaths per
1000 on program per year
|
|---|
|
Methadone
|
204
|
9300 (66%)
|
7.3 (range 6.9–7.5)
|
|
Buprenorphine
|
14
|
4800 (34%)
|
1.0 (range 0.63–1.5)
|
The sevenfold difference between methadone and buprenorphine death rates can be explained in part by the fact that buprenorphine is a partial agonist at opioid receptors, whereas methadone is a full opioid agonist and is more likely to cause respiratory depression in an overdose situation, especially when other depressant drugs are present.27 A recently published study from England and Wales found a similar result, with a relative risk ratio between methadone and buprenorphine of 6.23 (95% confidence interval [CI]: 4.79–8.10).28 Bell et al in New South Wales found a similar trend in 2009.29 One caveat on the Victorian data is that some of these deaths occurred in people who took syrup or tablets obtained from elsewhere and were not actual patients on the pharmacotherapy programs.
In 2007, Byrne and Wodak wrote that methadone should remain the drug of first choice because of its better rate of treatment retention, lower cost and reduced rate of illicit drug use.30 Ongoing evaluation studies since then (including a Cochrane review in 2014 of 31 trials) have demonstrated that patients on moderate (7–15 mg) to high (>16 mg) doses of buprenorphine have similar retention rates as those of methadone. These studies have also found that the two drugs are equivalent when measured by the outcomes of reducing drug use and criminal activities.31–33
The National guidelines for medication-assisted treatment of opioid dependence states that the choice between methadone or buprenorphine for opioid substitution treatment should be made in consultation with the patient, and informed by the patient’s preference and goals.34 In the authors’ opinion, the increasing evidence on risk ratios suggests that buprenorphine should be considered as the drug of first choice by clinicians when treating opioid dependence. This is especially so for polydrug users where overdose rates are high.27
Conclusion
Prescription drug abuse is a complex problem that needs to be addressed by society and the medical profession together. Doctors need to be aware of the risk of dependence and overdose with any drugs they prescribe, but particularly drugs of dependence. Opioids and benzodiazepines are associated with the highest risk of overdose deaths in Victoria. In a general practice setting, the use of evidence-based guidelines can help with managing inappropriate requests for drugs of dependence.
Patients need to be given information on the possible fatal complications of mixing opioids, benzodiazepines and/or alcohol. This information can enable them to reduce their own overdose risk by taking appropriate preventive action.
Regulatory changes in pharmaceutical medications can have an impact on patterns of drug prescribing and subsequent misuse. Implementation of real-time monitoring programs may assist doctors in making more appropriate prescribing decisions. Adequate strategies and resources need to be made available to manage the expected new cases of prescription drug abuse that would be detected by the real-time computer monitoring system. Suggested strategies in general practice for ameliorating the problem of prescription drug abuse are summarised in Box 1.
Box 1. Strategies for general practice for reducing or managing prescription drug abuse
- Drugs of dependence are the ones most likely to be abused. They are intended for short-term use (eg two to four weeks). If commenced following an acute hospital admission, a weaning off protocol should be provided or sought from the hospital staff or treating doctor6
- If drugs of dependence are required for longer term treatment, be clear of the diagnosis and monitor ongoing risks and benefits. The 4As of monitoring are analgesia, activities of daily living, adverse reactions and aberrant behaviours
- Develop a practice policy on reviewing patients on drugs of dependence. A number of helpful policies can be found on the RACGP website
- When reducing patients from long-term, high dose opioids, a step-wise reduction of 10% of the original dose per week is usually well tolerated with minimal psychological adverse effects. As the dose gets lower, the rate of reduction can vary from weekly to monthly36
- Learn how to respond to inappropriate requests for drugs of dependence. A number of helpful example responses to use in the consultation are available on the RACGP website
- An Australia-wide, 24 hour Prescription Shopping Information Service (1800 631 181) is available if you suspect a patient is seeking to obtain medicines in excess of therapeutic need
- A real-time computer monitoring system throughout Australia, when established, should help doctors manage their patients request for drugs more safely37
- Manage risk to patient and staff by stratifying patients into three groups depending on staff expertise, training and resources
- Managed at this general practice
- Managed at this general practice with specialist support
- Too complex for this general practice, needs specialist treatment
- Familiarise yourself with your local referral options for specialist services in drug and alcohol, chronic pain and mental health
- Participate in ongoing education of medical students and doctors on managing chronic conditions such as drug dependence and chronic pain
Further information can be found on the RACGP website (www.racgp.org.au/your-practice/guidelines/drugs-of-dependence-a)
|
Authors
Benny Monheit MBBS, MPH, FAChAM, Addiction Medicine Physician, Alfred Hospital and Southcity Clinic, Melbourne, Vic. bennymonheit@gmail.com
Danusia Pietrzak MBBS, General Practitioner with a special interest in addiction medicine, Southcity Clinic, Melbourne, Vic
Sandra Hocking RN Div1, Grad Dip Addiction, Drug and Alcohol Clinician, Southcity Clinic, Melbourne, Vic
Competing interests: None.
Provenance and peer review: Commissioned, externally peer reviewed.