The recent Grattan Institute report, entitled ‘Dying well’,1 highlights the current disconnect in Australia between people’s expressed wishes with regard to end-of-life care and what actually happens. If asked, most people have clear preferences regarding their end-of-life care;1 however, although hospitals and residential aged care facilities (RACFs) are usually the least preferred places to die,2 54% of people die in hospital and 32% in residential aged care.3 This seems to be because the open and systematic communication that is required to facilitate effective end-of-life planning occurs relatively infrequently.1 Advance care directives (ACDs) provide a way for people to plan ahead for a time when they have lost their decision-making capacity, in order to live well and die with dignity in accordance with their personal values.4 In Australia, however, the awareness and uptake of ACDs remains low;5–7 one survey of residential aged care facilities in regional New South Wales reported the presence of documented ACDs for only 5% of residents.8 This paper describes an approach to ACDs for patients in residential aged care.
Advance care planning and advance care directives
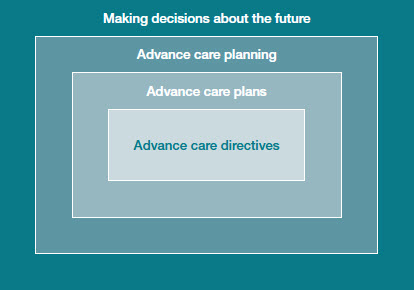 |
Figure 1. ‘Russian doll’ model of advance care directives and advance care planning
Adapted with permission from the Australian Health Ministers Advisory Council.
A National Framework for Advance Care Directives. Canberra: MHMAC, 2011. |
ACDs should be considered in the broader context of advance care planning (Figure 1). Advance care planning allows a person to plan for future health and personal care needs in case of becoming unable to make or communicate decisions. An advance care planning discussion allows a person’s individual values, beliefs and preferences to guide future decision making, and may result in a written advance care plan. An ACD is a special type of formal advance care plan, expressed in writing, signed by a competent adult and recognised by common law or legislation. Clinical care, treatment or resuscitation plans written by clinicians to guide clinical care should be informed by advance care plans and ACDs. Table 1 details the National Framework for Advance Care Directives4 Code for Ethical Practice for Advance Care Directives.
Table 1. The code for ethical practice for Advance Care Directives (ACDs)
|
- ACDs are founded on respect for a person’s autonomy and are focused on the person.
- Competent adults are autonomous individuals, entitled to make their own decisions about personal and health matters.
- Autonomy can be exercised in different ways according to the person’s culture, background, history or spiritual and religious beliefs.
- Adults are presumed competent.
- Directions in ACDs may reflect a broad concept of health.
- Directions in ACDs can relate to any future time.
- The person decides what constitutes quality of life.
- The substitute decision-maker has the same authority as the person when competent.
- The substitute decision-maker must honour residual decision-making capacity.
- The primary decision-making standard for substitute decision makers is substituted judgment.
- A substitute decision maker should only base his or her decision on best interests when there is no evidence of the person’s preferences on which to base substituted judgment.
- An ACD can be relied upon if it appears valid.
- A refusal of a health-related intervention in a valid ACD must be followed, if intended by the person to apply to the situation.
- A person, or their legally recognised substitute decision maker, can consent to treatment offered, refuse treatment offered, but cannot demand treatment.
- A valid ACD that expresses preferences or refusals relevant and specific to the situation at hand must be followed.
|
|
Adapted with permission from the Australian Health Ministers Advisory Council. A National Framework for Advance Care Directives. Canberra: MHMAC, 2011.
|
Types of ACDs
ACDs may record any of:4
- a person’s values, life goals and preferred outcomes
- directions about care and treatment refusals
- appointment of a substitute decision maker (SDM).
Legislation covering ACDs has been enacted in most Australian states and territories except New South Wales and Tasmania, where the common law applies.9 However, the name and nature of legislated instruments for each component of an ACD varies between jurisdictions.9 Clinicians should be familiar with the legal environment of the jurisdiction(s) in which they practice.
Case study
A man aged 88 years and legally blind, was brought regularly to his appointments by his daughter. He already has home care provided by the Department of Veterans’ Affairs. Two appointments ago, an advance care planning discussion was initiated, by raising the issue of higher level care and what he would like in the event he was no longer able to make decisions. He already had a form of ACD, having nominated his daughter to be a substitute decision maker, using the Power of Attorney instrument for his jurisdiction. Development of a more comprehensive advance care plan and consideration of other components of an ACD is still a work in progress. The daughter, also a patient, has expressed enormous relief and thanks on several occasions that the subject was raised.
Problems with ACDs
Problems with ACDs may occur when:4
- ACDs contain medical directions that are uninformed, too specific to account for changes in medical treatment, or too non-specific to guide decision making.
- SDMs are confused about their role and unsupported in decision making.
- People change their preferences over time but fail to update their ACD.
- Clinicians do not follow the directions in an ACD or respect the decision making of the SDM.
The substitute decision maker
It is important that any nominated SDM understands the responsibility to make the decision that they believe the person who has nominated them would make in the situation.4 This substitute decision should be based on what the SDM knows or can infer about the person’s life goals, views, values and beliefs in the context of information relevant to the situation, including medical advice. Only if there is no evidence of a person’s preferences on which to base a substituted decision should best interests be used in the decision-making process. In addition, any residual capacity of the person for whom a substituted decision is being made must be respected by the SDM.
Values, life goals and specific instructions
Problems with implementation of ACDs may arise if they contain medical directions that are either too specific or too vague to be useful. Where possible, statements expressing a person’s values, life goals and situations that would be unacceptable to the person should be incorporated into the ACD. These could include preferences to be accommodated (including residential decisions) and personal circumstances and functional outcomes that would be unacceptable. This assists any SDM, if appointed, in substituted decision making, and allows clinicians to make recommendations for medical care that respect the values expressed in the ACD.
Barriers to making advance directives
Many doctors find it difficult to talk with patients about end-of-life issues, resulting in delays in the discussion until death is imminent.10,11 Normalisation of the discussion is important10 and the National Framework for Advance Care Directives4 recommends that information about advance care planning and ACDs should become a routine part of patient contact with practitioners in health and aged care.
Establishing the patient’s cultural values and background is an important part of the advance care planning discussion. Many patients of minority cultural and language backgrounds are less likely to complete ACDs than the majority population12 and for some cultures, the principles of autonomy and individual decision making on which ACDs are based are quite foreign.13
A further barrier to making ACDs is time.10,14 The discussions required for effective and comprehensive advance care planning often do not fit neatly into the length of a standard consultation. However, with appropriate planning and discussion with the patient, appointments can be scheduled to allow the ACD to be completed. If the issue is raised in a timely fashion then usually there is no need for urgency. In practices where nursing staff assist in health assessments and management plans, training in the area of ACDs should be provided for nursing staff to facilitate their incorporation into routine assessment and management planning.
Resources for advance care planning and ACDs
There are many resources available to assist with advance care planning and making ACDs. The following are recommended:
Advance Care Planning Australia has a website that includes links to training resources and courses provided by the Respecting Patient Choices Program at Austin Health. http://advancecareplanning.org.au/
Caresearch, a national palliative care information service hosted by Flinders University, provides extensive information on palliative care topics including advance care planning, and has a specific hub for GPs. www.caresearch.com.au/ caresearch/ ProfessionalGroups/ GPHome/ tabid/ 901/ Default.aspx
Decision Assist, an Australian Government–funded specialist advice phone line for GPs and aged care providers, available 24/7 for palliative care advice and 8am until 8pm for advance care planning advice. In addition, the website has many useful fact sheets and educational resources. Phone 1300 668 908. www.decisionassist.org.au
Considerations for ACDs for patients in residential care
During a review of quality of advance care policy and practice in aged care facilities in Victoria, Silvester et al15,16 developed a set of best practice principles for advance care planning in residential aged care facilities (Table 2). These are consistent with the best practice principles in the National Framework for Advance Care Directives.4
Table 2. Overview of best practice advance care planning
in residential aged care facilities
|
- Facilities have readily accessible written policies and procedures about advance care planning, with advance care planning as a routine component of care.
- Regular education on advance care planning is provided to aged care staff, residents and relatives and general practitioners (GPs).
- Residents and families are given information regarding advance care planning before or at admission.
- Advance care planning is offered to residents within 28 days of admission.
- Advance care planning is completed by an appropriately skilled healthcare professional during an in-depth discussion with the resident and/or their family.
- The conversation focuses on reasonable outcomes and “living well”, raising the issues of life-prolonging treatment generally without focusing on any specific treatment.
- GPs are involved in any advance care planning discussions.
- Completed plans are regularly reviewed.
- Advance care planning documents clearly specify: a nominated SDM where applicable, current state of health, values and beliefs, future unacceptable health conditions, level of preferred medical treatment indicated, any specific wanted/unwanted treatments, goals for end of life care, appropriate signatures, evidence of GP review.
- Facilities have effective information transfer systems that enable communication of advance care planning information to other health care providers.
|
|
Adapted with permission from BMJ Publishing Group Ltd from Silvester W, Fullham RS, Parslow, et al. Quality of advance care planning policy and practice in residential aged care facilities in Australia. BMJ Support Palliat Care 2013;3:349–57.
|
Prior to admission
Many patients have lost cognition by the time they are admitted to residential care.17 Advance care planning and the opportunity to make an ACD are important components of routine care for any patient with a chronic illness likely to progress to a need for residential care. In particular, if a patient has high-level needs and is being considered for home care services, this should trigger a review of their advance care plan.1 Patients of advancing age who are well should also have this opportunity as part of their routine healthcare. General practitioners (GPs) are in an ideal position to provide this, as the majority of older patents visit a GP at least once per year.18
On admission to residential care
Admission to residential care provides a further opportunity to review any advance care plan and ACD. Ideally, residential care facilities (RCFs) will have policies, procedures and regular educational activities to ensure that appropriate review occurs as part of routine practice15,16,19,20 (Table 2, items 1–4). It is important that GPs are involved in these discussions (Table 2, item 7).
Triggers for review
Any change in residential or healthcare status should lead to a review of the advance care plan and any ACD. In addition, routine scheduled review should occur (Table 2, item 8). This could be facilitated by computer-generated automatic reminders, similar to those used for other aspects of routine preventive care.
Documentation and transfer of information
It is important that the presence of any advance care plan or ACD is documented by the RACF and by the GP, and that systems are in place to ensure this information transfers with the patient, should they require care in another facility (Table 2, item 10). Australia’s personally controlled eHealth record allows a patient to record the location of an ACD.21 In addition, the SDM should hold a copy of the ACD in order to be able to provide it if required.
An approach to decision making for patients with an ACD
Table 3 provides a suggested decision-making pathway for patients with impaired capacity and an ACD.
Table 3. Suggested decision-making pathway for a
patient with an ACD
|
|
Step 1
|
Assess capacity to make the decision required –
if substitute decision required proceed to step 2
|
|
Step 2
|
Establish whether preferences relevant to the situation have been previously expressed as an ACD or in previous discussions
|
|
Step 3
|
For health-related decisions consider clinician advice about treatment options and likely outcomes in light of the person’s wishes, including interventions considered overly burdensome or intrusive and outcomes to avoid
|
|
Step 4
|
Respect specific refusals of medical treatments and interventions if intended to apply to the current circumstances
|
|
Step 5
|
Give particular weight to other preferences and directions in the ACD relevant to the current decision
|
|
Step 6
|
If no specific relevant preferences and directions consult with others close to the person to determine relevant previously expressed views and social or relationship factors the person would consider in decision making
|
|
Step 7
|
Consider the person’s known values, life goals and cultural, linguistic, spiritual and religious preferences, and aim to make the decision that the person would make with the same information and advice
|
|
Step 8
|
Where several treatment options satisfy these decision-making criteria, choose the least restrictive option that best ensures the person’s proper care and protection
|
|
Step 9
|
For residential decisions, consider whether existing informal arrangements for the person’s care are adequate and the desirability of not disturbing those arrangements
|
|
Step 10
|
If there is no evidence of what the person would have decided, make the decision that best protects the person’s personal best interests
|
|
Adapted with permission from the Australian Health Ministers Advisory Council.
A National Framework for Advance Care Directives. Canberra: MHMAC, 2011.
|
Conclusions
Most people have clear preferences with regard to end-of-life care; however in practice these preferences frequently are not followed. ACDs allow people to record their preferences in advance of any loss of decision-making capacity. The opportunity to make an ACD should be offered to everyone as part of routine healthcare, well in advance of any need for residential care. However once residential care is required, ACDs become even more important. Clinicians and RACFs should take a systematic approach to ACDs that ensures routine assessment and review of ACDs and facilitates transfer of information held in ACDs between healthcare providers.
Key points
- Initiating the discussion is often the most difficult, but also the most important step.
- Where possible, and consistent with the patient’s wishes, involve family and, in particular, any SDM in the discussion.
- The opportunity to make an ACD should be part of routine care for all patients in residential care.
- To maintain relevance, review of ACDs should occur on a regular, scheduled basis and also with any change in health or residential status.
- Communication of any ACD to all relevant healthcare providers is essential to ensure that ongoing care is congruent with the patient’s wishes.
- Resources are available to facilitate advance care planning, including making ACDs.
Competing interests: None.
Provenance and peer review: Commissioned, externally peer reviewed.